PPG Waveform: Anatomy, Features, and Clinical Meaning
The PPG waveform encodes far more than heart rate. Learn the anatomy of each pulse wave, what dicrotic notch position means, and how waveform shape reveals cardiovascular health.
A single PPG waveform — one pulse cycle from foot to foot — contains a rich anatomical fingerprint of the cardiovascular system. The timing, shape, and relative amplitudes of its features reflect arterial stiffness, peripheral vascular resistance, cardiac contractility, and autonomic tone. Extracting this information is the difference between a basic heart rate tracker and a clinical-grade cardiovascular monitor.
This guide walks through the full anatomy of the PPG pulse waveform, explains what each feature represents physiologically, and shows how waveform shape changes across age, disease, and hemodynamic state.
The Anatomy of a Single PPG Pulse
A normal PPG pulse waveform — viewed as a single beat plotted over time — has a characteristic shape with several identifiable landmarks:
Foot (Onset, Minimum)
The lowest point of the waveform, occurring at end-diastole just before the next systolic ejection. The "foot" of successive beats is used to calculate inter-beat intervals (IBIs) with higher precision than peak-to-peak timing, because the foot has a steeper, more reliable edge.
Systolic Upstroke
The rapid rise from foot to systolic peak. Its slope reflects cardiac contractility and the speed of pulse wave propagation. A steep, fast upstroke indicates vigorous cardiac output and low arterial stiffness. In cardiac dysfunction or severe vasospasm, the upstroke becomes more gradual.
Systolic Peak (P1)
The first and usually highest peak, occurring approximately 100–180 ms after the ECG R-wave (at resting heart rates). Its absolute amplitude is proportional to stroke volume and peripheral vascular resistance — but only relatively, since the PPG signal is not calibrated to pressure units.
Incisura / Dicrotic Notch
A small inflection or dip on the descending limb of the waveform, occurring when the aortic valve closes (aortic valve closure, or AVC). This is one of the most clinically informative features of the PPG waveform.
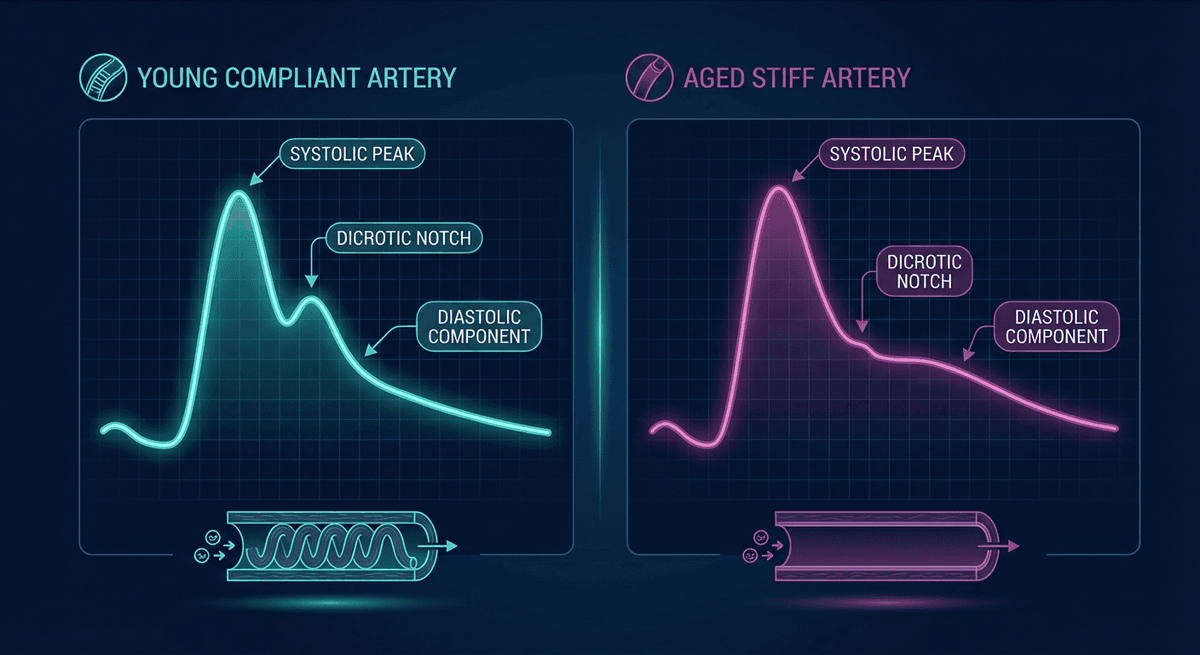
In young, healthy adults with compliant arteries, the notch appears clearly defined and positioned in the lower third of the descending limb. As arterial stiffness increases — with age, hypertension, diabetes, or cardiovascular disease — the notch moves upward and becomes less distinct. In the elderly or in patients with severe arterial stiffness, the notch may disappear entirely into a smooth, monotonic descent.
Diastolic Peak (P2)
The secondary peak that follows the dicrotic notch, representing the reflected pressure wave returning from the periphery (primarily from the lower body and bifurcation of the aorta). Its relative height compared to P1 (expressed as the augmentation index, AIx) is a validated marker of arterial stiffness and cardiovascular risk.
In young, healthy individuals with compliant vessels, P2 is substantially lower than P1. In older individuals or those with stiffened arteries, reflected waves return faster (because pulse wave velocity is higher), arriving during systole rather than diastole and augmenting P1 — pushing AIx higher.
Diastolic Descent and Return to Foot
The waveform descends after P2 back to the foot level. The rate and shape of this descent reflect peripheral resistance and venous capacitance.
Key Waveform Feature Definitions
| Feature | How Measured | Clinical Meaning |
|---|---|---|
| Pulse width (PW) | Time from foot to foot | Reflects heart rate |
| Systolic upstroke time (UT) | Time from foot to P1 | Cardiac contractility, arterial compliance |
| Peak-to-peak amplitude | Height of P1 above foot | Perfusion quality, cardiac output (relative) |
| Augmentation index (AIx) | (P2 − P1) / (P1 − foot) × 100 | Arterial stiffness, wave reflection |
| Reflection index (RI) | P2 amplitude / P1 amplitude | Peripheral vascular tone |
| Time to diastolic peak (T2) | Time from foot to P2 | Pulse wave velocity (inverse relationship) |
| Diastolic time fraction (DTF) | Diastolic time / total pulse period | Myocardial perfusion opportunity |
| Large arterial stiffness index (SI) | Body height / time between P1 and P2 | Aortic pulse wave velocity proxy |
How Waveform Shape Changes With Age
One of the most consistent and well-studied changes in the PPG waveform is its transformation with aging.
In a 20-year-old with healthy arteries, the waveform typically shows: a sharp, fast upstroke; a clear P1 peak; a well-defined dicrotic notch positioned in the lower half of the descending limb; and a P2 clearly below P1.
By age 60 in a typical individual: the upstroke is slower; the notch has moved upward and blurred; P2 may equal or exceed P1; the waveform appears "stiffer." This happens because pulse wave velocity in the aorta increases from roughly 5–8 m/s in young adults to 10–15 m/s in the elderly. Reflected waves that used to arrive during diastole now arrive during late systole, augmenting the systolic pressure — a mechanism that contributes directly to isolated systolic hypertension.
This age-related waveform change has been characterized quantitatively in large population studies. The Asklepios cohort study (n=2524) and the PARADIGM-HF analysis both used PPG-derived vascular aging scores. See our more detailed guide to PPG vascular age assessment for clinical applications.
Disease States That Alter Waveform Shape
Hypertension
Elevated blood pressure accelerates arterial stiffening. The PPG waveform in hypertensive patients shows an upward-shifted dicrotic notch, elevated AIx, and a P2 that often approaches or exceeds P1 even at younger ages. Chronic hypertension eventually produces a smooth, rounded waveform with loss of the diastolic peak definition.
Atrial Fibrillation
AF produces a rhythmically irregular sequence of waveforms with highly variable amplitudes. The amplitude variation occurs because different R-R intervals mean different diastolic filling times — short intervals produce smaller strokes, longer intervals produce larger strokes. This beat-to-beat amplitude modulation is the basis for AF detection algorithms in wearables. Learn more in our PPG AF screening guide.
Heart Failure
In decompensated heart failure, the waveform typically shows reduced amplitude (low stroke volume), prolonged upstroke time (reduced contractility), and sometimes alternating waveform heights (pulsus alternans) — a sign of severe dysfunction. The dicrotic notch may be absent in severe low-output states.
Sepsis
Early septic shock produces a characteristic high-amplitude, bouncy PPG waveform with a prominent dicrotic notch and increased diastolic component — reflecting systemic vasodilation and high cardiac output. As sepsis progresses and myocardial depression sets in, the waveform transitions toward low amplitude.
Second Derivative PPG (SDPPG or APG)
The second derivative of the PPG waveform (called SDPPG or accelerated plethysmogram, APG) amplifies subtle differences in waveform morphology that are hard to see in the raw signal. It reveals five distinct waves labeled a through e:
- a wave: Rapid systolic increase in the early systolic phase
- b wave: Deceleration of systolic upstroke
- c wave: Second increase related to reflected wave from the lower body
- d wave: Deceleration of reflected wave
- e wave: Diastolic component
The ratios of these waves — particularly the b/a and d/a ratios — have been used in Japanese and Korean research traditions as vascular aging indices, though their clinical adoption in Western medicine has been limited. For a complete treatment, see our PPG second derivative (SDPPG) guide.
Extracting Waveform Features in Practice
Waveform morphology analysis requires several preprocessing steps:
- Segment individual beats: Use beat detection (onset-to-onset) to extract individual pulse cycles.
- Normalize: Either time-normalize to a standard length (for template comparison) or preserve absolute timing (for PTT, contractility indices).
- Compute landmarks: Locate P1 using peak detection; locate the dicrotic notch using algorithms based on the second derivative minimum or inflection detection; locate P2 using post-notch peak detection.
- Handle edge cases: Some waveforms (especially in elderly patients) have no distinct notch. Algorithms must handle missing features gracefully.
Software like ChatPPG's algorithm suite handles this automatically, but understanding the underlying anatomy helps interpret results.
Frequently Asked Questions
What is the dicrotic notch in a PPG waveform? The dicrotic notch is a small dip on the descending limb of the PPG pulse waveform, occurring when the aortic valve closes. It represents the brief reversal of aortic flow at end-systole. Its position, depth, and clarity are indicators of arterial stiffness — it is more distinct and lower on the waveform in young, healthy individuals.
What does a high augmentation index (AIx) mean? A high AIx means the reflected wave from the periphery arrives during systole and augments the systolic peak. This happens when arteries are stiff and pulse waves travel fast. AIx above ~30% in middle-aged adults is associated with increased cardiovascular risk. Normal ranges vary with age, sex, and heart rate.
Does PPG waveform shape change with exercise? Yes, significantly. During exercise, heart rate increases (shortening pulse period), peripheral vasodilation increases waveform amplitude, and the diastolic-to-systolic peak ratio changes. The dicrotic notch may become less prominent at high heart rates. Waveform morphology analysis in exercise conditions requires separate normative references.
Can PPG detect blood pressure from waveform shape? Cuffless blood pressure estimation using PPG waveform features is an active research area. Current approaches use pulse transit time, augmentation index, and systolic upstroke time — all calibrated against reference BP measurements. No current method is accurate enough for unsupervised clinical use without calibration, but the technology is advancing rapidly. See our PPG blood pressure estimation guide.
What does a "poor quality" PPG waveform look like? Artifact-contaminated waveforms show irregular peaks, rapid amplitude fluctuations, peaks at non-physiological frequencies, and loss of the characteristic rise-and-fall shape. Quality assessment algorithms automatically flag such segments to prevent spurious measurements.
How many beats are needed for accurate waveform feature analysis? For stable resting measurements, 30–60 consecutive beats is a practical minimum. For HRV analysis, 5 minutes of clean data is standard. For single-beat morphology indices like AIx, one averaged beat from multiple cycles is used, requiring at least 30 beats for stable averaging.
References
-
Millasseau, S. C., Ritter, J. M., Takazawa, K., & Chowienczyk, P. J. (2006). Contour analysis of the photoplethysmographic pulse measured at the finger. Journal of Hypertension, 24(8), 1449–1456. https://doi.org/10.1097/01.hjh.0000239277.05068.85
-
Takazawa, K., Tanaka, N., Fujita, M., et al. (1998). Assessment of vasoactive agents and vascular aging by the second derivative of photoplethysmogram waveform. Hypertension, 32(2), 365–370. https://doi.org/10.1161/01.HYP.32.2.365
-
Charlton, P. H., et al. (2022). Wearable photoplethysmography for cardiovascular monitoring. Proceedings of the IEEE, 110(3), 355–381. https://doi.org/10.1109/JPROC.2022.3149785
-
Wilkinson, I. B., & Webb, D. J. (2001). Venous occlusion plethysmography in cardiovascular research: methodology and clinical applications. British Journal of Clinical Pharmacology, 52(6), 631–646. https://doi.org/10.1046/j.0306-5251.2001.01495.x