Pulse Scale Grading System: 0 to 3+ Scale, Palpation Technique, and PPG Comparison
How to use the 0 to 3+ pulse grading scale for clinical assessment. Covers palpation technique at each site and PPG-based objective alternatives.
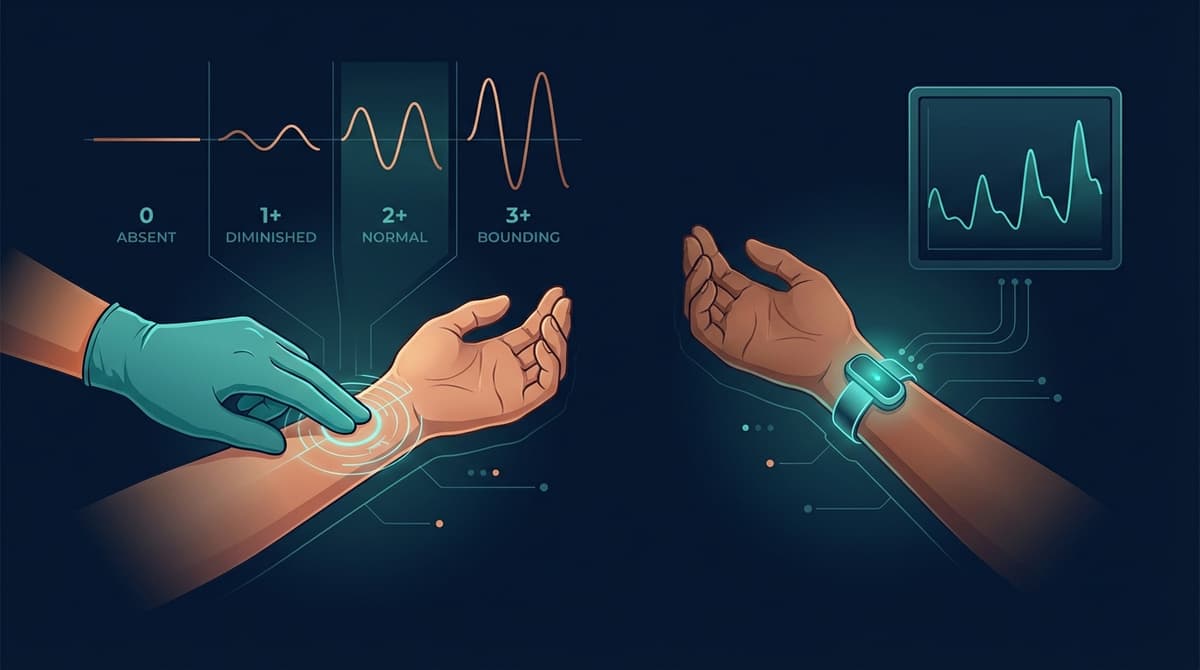
The pulse grading scale is a standardized 0 to 3+ system used by clinicians to document the strength of a peripheral pulse during physical examination. A grade of 0 means the pulse is absent and cannot be felt. A grade of 1+ indicates a diminished or barely palpable pulse. A grade of 2+ represents a normal, expected pulse that is easily felt. A grade of 3+ describes a bounding pulse, one that is abnormally strong and easily palpable with minimal pressure. This scale provides a common language for clinicians to communicate vascular status, but it remains inherently subjective. Photoplethysmography (PPG) now offers an objective, continuous alternative through metrics like perfusion index and pulse amplitude, which quantify the same vascular characteristics that palpation attempts to assess by feel.
Understanding the 0 to 3+ Pulse Grading Scale
The 0 to 3+ scale is the most widely used system in nursing and medical practice, though some institutions use a 0 to 4+ variant. The four-point version used here is endorsed by major clinical nursing references and vascular surgery guidelines.
Grade 0: Absent Pulse
No pulse is detectable at the assessment site. This finding may indicate complete arterial occlusion, severe peripheral artery disease, or improper palpation technique. Before documenting a grade of 0, clinicians should ensure correct anatomical placement, adequate palpation pressure, and warm ambient conditions. A Doppler ultrasound probe or PPG sensor should be used to confirm truly absent flow, since even experienced practitioners sometimes fail to locate pulses that are present but faint.
Grade 1+: Diminished Pulse
The pulse is palpable but weak, often described as thready or difficult to find. It may disappear with slight changes in finger pressure. A diminished pulse can reflect reduced cardiac output, increased peripheral vascular resistance, hypovolemia, or partial arterial obstruction. In patients with peripheral artery disease, a 1+ pulse distal to a stenosis is a common finding.
Grade 2+: Normal Pulse
The pulse is readily palpable with normal finger pressure. It is the expected finding in healthy individuals with intact vascular supply. A 2+ pulse has a smooth, regular upstroke and a clear, reproducible rhythm. This is the baseline against which all other grades are compared.
Grade 3+: Bounding Pulse
The pulse is abnormally strong and easily felt, sometimes visible without palpation. Bounding pulses are associated with high cardiac output states such as fever, sepsis, anemia, hyperthyroidism, aortic regurgitation, and exercise. They can also occur with arteriovenous fistulas or after administration of vasodilatory medications. While a bounding pulse is not always pathological, it warrants clinical investigation when it appears outside of expected contexts.
Palpation Technique by Anatomical Site
Proper technique is the foundation of reliable pulse assessment. The examiner should use the pads of the index and middle fingers, never the thumb (which has its own palpable pulse). Pressure should start light and increase gradually. Each pulse should be assessed for rate, rhythm, strength, and symmetry.
Radial Artery
The radial pulse is the most commonly assessed peripheral pulse. Locate it on the flexor surface of the wrist, just lateral to the flexor carpi radialis tendon. Place two fingertips gently over the artery and apply light to moderate pressure. The radial pulse is typically easy to find and serves as the default site for routine heart rate checks and initial vascular assessments.
Dorsalis Pedis Artery
This pulse is found on the dorsum of the foot, lateral to the extensor hallucis longus tendon. It runs roughly between the first and second metatarsals. The dorsalis pedis pulse is congenitally absent in approximately 5 to 10% of healthy individuals (Mowlavi et al., 2002; DOI: 10.1016/S0741-5214(02)00073-3), so its absence alone does not confirm vascular disease. Always compare with the posterior tibial pulse on the same side.
Posterior Tibial Artery
Palpate this pulse posterior and inferior to the medial malleolus, in the groove between the medial malleolus and the Achilles tendon. Cup the heel with your hand and wrap your fingers around to the medial ankle. This site is essential for lower extremity vascular assessment and is generally more reliably present than the dorsalis pedis.
Femoral Artery
The femoral pulse is located at the midinguinal point, midway between the anterior superior iliac spine and the pubic symphysis. It requires firmer pressure than distal sites due to overlying tissue. The femoral pulse is valuable for assessing proximal vascular disease and is typically one of the last pulses to disappear in severe hypotension or cardiac arrest.
Carotid Artery
Palpate the carotid pulse in the anterior triangle of the neck, between the trachea and the sternocleidomastoid muscle, at the level of the thyroid cartilage. Assess one side at a time, never both simultaneously, to avoid reflex bradycardia from carotid sinus stimulation. The carotid pulse is the preferred site during cardiopulmonary resuscitation because it persists even in very low cardiac output states.
Clinical Significance of Changes in Pulse Grade
Serial pulse grading is far more informative than a single measurement. A change from 2+ to 1+ at the dorsalis pedis after vascular surgery may signal graft occlusion or embolization and demands immediate evaluation. A bilateral shift from 2+ to 3+ in the setting of fever suggests a hyperdynamic circulatory state.
Asymmetry between left and right pulses is also clinically significant. A unilaterally diminished radial pulse may indicate subclavian steal syndrome, thoracic outlet syndrome, or aortic dissection. Comparison of upper and lower extremity pulse grades helps screen for aortic coarctation, where arm pulses are bounding while femoral and pedal pulses are diminished or absent.
In postoperative patients, particularly after cardiac catheterization, orthopedic procedures, or vascular interventions, pulse checks at regular intervals are standard of care. The pulse grade serves as an early warning for compartment syndrome, arterial thrombosis, and limb ischemia.
Limitations of Subjective Pulse Grading
Despite its widespread use, manual pulse grading has well-documented shortcomings. Inter-rater reliability is poor. Studies have shown that two clinicians examining the same patient often disagree on the pulse grade, particularly at the boundary between 1+ and 2+. Brearley et al. (1992; DOI: 10.1016/0741-5214(92)90018-4) found that agreement between experienced vascular surgeons on pedal pulse assessment was only moderate, with kappa values around 0.3 to 0.5.
Factors that degrade palpation accuracy include cold ambient temperature (causing vasoconstriction), patient obesity, edema overlying the artery, examiner fatigue, and the inherent difficulty of calibrating subjective finger pressure against a standardized scale. There is no way to verify the accuracy of a palpated grade against a true reference standard in real time, and documentation is limited to ordinal categories that cannot capture the continuous nature of pulse strength.
PPG as an Objective Pulse Assessment Tool
Photoplethysmography measures the optical absorption changes caused by pulsatile arterial blood flow in tissue. The resulting PPG waveform encodes the same vascular information that clinicians attempt to assess through palpation, but it does so with quantitative precision and continuous recording capability.
Perfusion Index as a Continuous Pulse Grade
The perfusion index (PI) is the ratio of the pulsatile (AC) component of the PPG signal to the non-pulsatile (DC) component, expressed as a percentage. A high PI indicates strong pulsatile flow (analogous to a 2+ or 3+ pulse), while a very low PI indicates weak or absent pulsatile flow (analogous to a 0 or 1+ pulse).
Typical PI values at the fingertip range from 0.02% (barely detectable flow) to over 20% (very strong pulsatile flow). Unlike ordinal pulse grades, PI provides a continuous numeric value that enables precise trending over time. A PI dropping from 5.0 to 1.2 over two hours communicates far more information than a transition from "2+" to "1+" documented in a nursing assessment.
Pulse Amplitude and Waveform Morphology
Beyond PI, the raw amplitude of the PPG waveform and its morphological features provide additional vascular information. A waveform with a sharp systolic upstroke and a clear dicrotic notch suggests compliant arteries and normal vascular tone. Flattened, delayed, or damped waveforms may indicate proximal stenosis, reduced cardiac output, or increased vascular stiffness.
PPG sensors placed at multiple anatomical sites can simultaneously assess bilateral symmetry and proximal-to-distal perfusion gradients. This approach eliminates the sequential, memory-dependent nature of manual pulse comparison.
Advantages Over Manual Grading
PPG-based assessment offers several concrete advantages over palpation. First, it is objective and reproducible: two PPG sensors on the same site will produce nearly identical readings. Second, it is continuous: PPG can monitor perfusion every heartbeat for hours or days without operator involvement. Third, it is quantitative: changes can be tracked numerically and graphed over time. Fourth, it works in situations where palpation fails. Obese patients, edematous limbs, and cold extremities that frustrate manual assessment can still yield usable PPG signals with appropriate sensor placement and contact pressure optimization.
PPG does not replace the clinical judgment that accompanies manual examination, but it provides the data layer that manual grading has always lacked.
Clinical Integration
Modern pulse oximeters already display PI alongside SpO2 and heart rate, making PPG-based perfusion assessment immediately available at the bedside. Wearable devices equipped with PPG sensors are beginning to provide continuous peripheral perfusion monitoring outside the hospital. As these technologies mature, the 0 to 3+ scale may evolve from a primary assessment tool to a rapid screening method, backed by quantitative PPG data whenever precision matters.
Frequently Asked Questions
What does a 2+ pulse mean?
A 2+ pulse is a normal finding indicating that the pulse is easily palpable with standard finger pressure. It represents adequate arterial blood flow to the assessed site and is the expected grade in healthy individuals. There is no need for further vascular workup when pulses are symmetrically 2+ at all sites.
What is the difference between a 1+ and 3+ pulse?
A 1+ pulse is diminished, meaning it is weak and difficult to feel. It may indicate reduced blood flow due to arterial narrowing, low cardiac output, or vasoconstriction. A 3+ pulse is bounding, meaning it is abnormally strong. Bounding pulses are typically seen in high-output states such as fever, anemia, or aortic valve regurgitation. Both findings warrant clinical investigation.
How reliable is manual pulse grading between different examiners?
Manual pulse grading has moderate inter-rater reliability at best. Studies report kappa values between 0.3 and 0.5 for pedal pulse assessment among experienced clinicians. Disagreements are most common at the 1+ to 2+ boundary. Factors such as examiner experience, patient anatomy, and environmental temperature all influence palpation results. PPG-based perfusion index offers a more reproducible alternative.
Can PPG replace manual pulse palpation?
PPG can supplement and quantify what palpation assesses, but it does not fully replace the physical examination. Palpation provides immediate, equipment-free information about pulse rate, rhythm, and character that informs bedside clinical reasoning. PPG excels at continuous monitoring, objective trending, and detecting perfusion changes that are too subtle for fingers to perceive. The best practice is to combine both methods.
What is a normal perfusion index value on a PPG device?
Perfusion index at the fingertip typically ranges from 1.0 to 20.0 in healthy adults at rest, with a median around 3.0 to 5.0. Values below 0.5 to 1.0 may indicate poor peripheral perfusion and roughly correspond to a 1+ or absent palpable pulse. PI varies significantly with temperature, body site, and individual physiology, so trending within a single patient is more informative than comparing against fixed cutoffs.
Why might a pulse be absent (grade 0) on palpation but detectable with PPG?
A PPG sensor can detect very weak pulsatile flow that falls below the threshold of human tactile perception. In patients with severe vasoconstriction, peripheral vascular disease, or edema, the arterial pulsation may be too faint or too deep for fingers to feel. PPG's optical detection method is not limited by tissue depth or tactile sensitivity in the same way, though very low perfusion states can still challenge PPG signal quality.
How often should peripheral pulses be assessed postoperatively?
Assessment frequency depends on the surgical procedure and clinical context. After vascular surgery or cardiac catheterization, pulses are typically checked every 15 minutes for the first hour, then every 30 minutes for two hours, then hourly. After orthopedic procedures with tourniquet use or fracture fixation, hourly pulse checks for the first 12 to 24 hours are standard. Continuous PPG monitoring can supplement these interval checks and provide real-time alerts for sudden perfusion changes.