PPG Pulse Pressure Variation Noninvasive Monitoring: Can Pleth Variability Guide Fluid Response?
PPG pulse pressure variation monitoring estimates respiratory-linked hemodynamic variability noninvasively, but its value depends on ventilation, rhythm, and signal quality.
PPG pulse pressure variation monitoring uses respiratory changes in the pleth waveform to estimate whether a patient may respond to fluids. It is attractive because it offers a noninvasive window into hemodynamics, but its value depends heavily on context, especially ventilation pattern, cardiac rhythm, and peripheral vascular tone.
Definition box: Pulse pressure variation is the respiratory swing in arterial pulse pressure. In PPG systems, related indices use pulse amplitude variability as a noninvasive surrogate.
This topic sits at the intersection of physiology and signal interpretation. Clinicians want to know whether a patient is fluid responsive. PPG offers a clue, not a final answer.
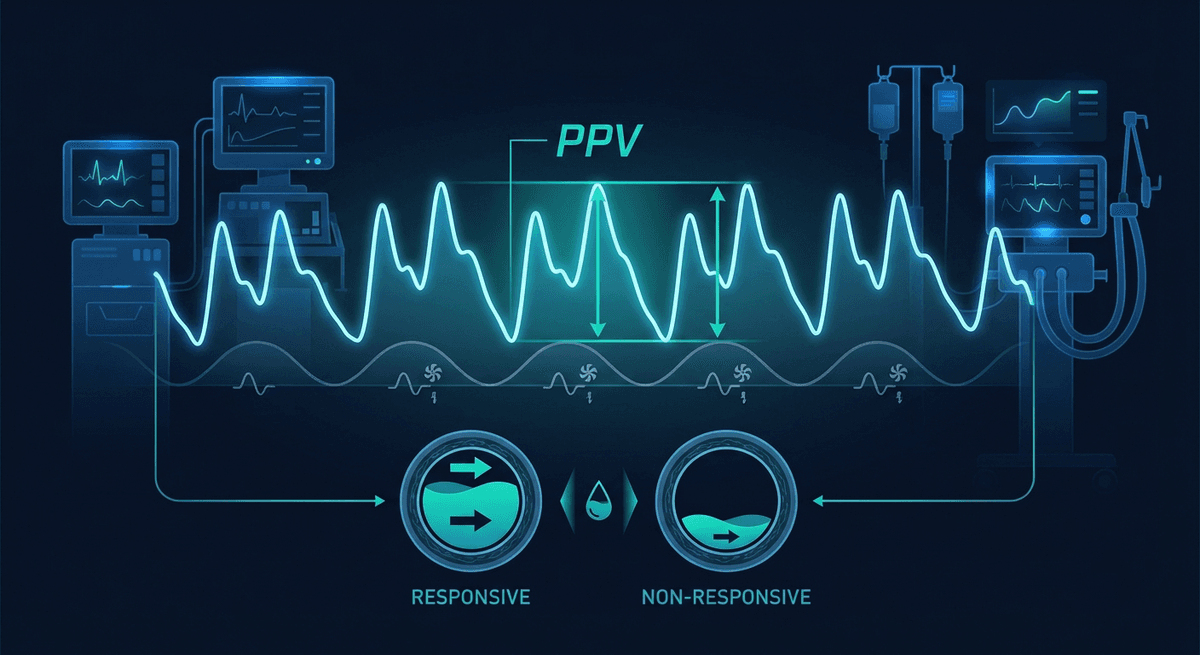
How respiratory variation shows up in the PPG waveform
During positive-pressure ventilation, intrathoracic pressure shifts venous return and ventricular loading across the respiratory cycle. If the patient is preload responsive, stroke volume changes more dramatically breath to breath. That hemodynamic swing can show up as variation in pleth waveform amplitude.
This is the physiological logic behind pleth variability metrics.
The key idea is simple:
- stronger respiratory amplitude swings may suggest preload dependence
- smaller swings may suggest less fluid responsiveness
But the peripheral optical waveform is not the same as a central invasive pressure waveform. It also reflects vasomotor tone, local perfusion, and measurement site effects.
Is PPG variation the same as invasive arterial PPV?
No. The terms are closely related, but they should not be treated as interchangeable.
An arterial line directly measures pressure at high fidelity. A pleth waveform measures optical changes tied to pulsatile blood volume. Those are related signals, but not identical ones.
That distinction matters because PPG can be distorted by:
- vasoconstriction
- sensor site choice
- motion
- contact pressure
- ambient interference
For foundational context, see PPG vs ABP comparison and PPG waveform basics.
When does noninvasive pleth variability work best?
This is the most important practical question.
Controlled mechanical ventilation
Predictive performance is best when the patient is fully ventilated with regular tidal volumes and minimal spontaneous respiratory effort.
Regular cardiac rhythm
Atrial fibrillation and frequent ectopy disrupt beat-to-beat consistency, making respiratory interpretation much harder.
Stable vasomotor state
Severe vasoconstriction or vasoactive drug shifts can change pleth amplitude independently of fluid responsiveness.
Good signal quality
Weak or noisy waveforms reduce trust immediately.
In other words, pleth variability works best in a controlled environment, not a chaotic one.
Where does it struggle?
Spontaneously breathing patients
Breath size and timing vary, so respiratory amplitude swings are less standardized.
Low tidal volume ventilation
Smaller intrathoracic pressure shifts reduce the signal of interest.
Arrhythmia
Irregular filling patterns make respiratory variability harder to isolate.
Peripheral hypoperfusion
The optical signal may be too unstable to interpret.
Open-chest and unusual surgical conditions
The normal cardiopulmonary mechanics underlying PPV assumptions can break down.
These are not edge cases. They are common reasons PPG hemodynamics fail in practice.
Why this still matters clinically
Even with those limits, a noninvasive fluid responsiveness clue is valuable.
Perioperative monitoring
During surgery, pleth variability can add context when the clinician is deciding whether hypotension is fluid-responsive or more related to vasodilation, anesthetic depth, or bleeding.
Step-down and monitored wards
If a patient does not have an arterial line, noninvasive trends may still help frame escalation decisions.
Procedure suites
Short cases with controlled ventilation are one of the cleaner environments for this technology.
This overlaps with ideas discussed in PPG perioperative monitoring and PPG anesthesia depth monitoring, although the signal target is different.
How should clinicians interpret a high pleth variability signal?
Carefully. A high value does not automatically mean give fluid.
The right interpretation asks:
- Is the patient mechanically ventilated?
- Is rhythm regular?
- Is the waveform clean?
- Could vasoconstriction be driving the amplitude change?
- Is the patient likely fluid tolerant?
Fluid responsiveness is not the same as fluid need. A patient can be fluid responsive and still not benefit from extra fluid if pulmonary edema or cardiac dysfunction is the bigger problem.
What is the best role for wearable or noninvasive PPG here?
Right now, the strongest role is monitored clinical settings rather than consumer wearables. The physiology is real, but the assumptions are strict. A wrist device on a walking patient is not the right tool for pleth variability-guided fluid management.
Still, the broader lesson matters: respiratory modulation of the PPG waveform contains hemodynamic information. As sensing improves, more of that information may become clinically usable.
FAQ
What is noninvasive pulse pressure variation with PPG?
It is the use of respiratory-linked changes in the pulse waveform to estimate whether stroke volume may respond to fluid administration.
Is PPG pulse pressure variation the same as arterial line PPV?
No. PPG-based variability is related, but it is not identical to invasive arterial pulse pressure variation and can be affected by peripheral vascular tone.
When does pleth variability work best?
It works best in controlled mechanical ventilation with regular rhythm, stable tidal volumes, and clean signal conditions.
Can it be used in spontaneously breathing patients?
Its performance is weaker in spontaneous breathing because respiratory mechanics are less standardized and waveform variability is harder to interpret.
Why do clinicians care about this metric?
Because it may help identify fluid responsiveness without placing an arterial line, especially in perioperative or monitored acute care settings.
PPG variation versus pleth variability index
People often use these terms loosely, but the details matter. Pleth variability index is a proprietary or semi-proprietary style of derived metric in some monitoring systems. More broadly, clinicians and researchers may analyze respiratory variation in pulse amplitude using different formulas, preprocessing choices, and exclusion rules.
That means results are not always interchangeable across vendors or studies. Two devices may both claim to reflect fluid responsiveness, yet derive the number differently.
Why vascular tone complicates interpretation
This is one of the biggest reasons the pleth waveform is not the same as arterial pressure. If vasoconstriction changes the local optical amplitude, the measured variability may shift even when true stroke-volume responsiveness has not changed much. That is a problem in shock states, anesthesia, and vasoactive medication use.
The physiology is real. The confounding is real too.
Frequently Asked Questions
- What is noninvasive pulse pressure variation with PPG?
- It is the use of respiratory-linked changes in the pulse waveform to estimate whether stroke volume may respond to fluid administration.
- Is PPG pulse pressure variation the same as arterial line PPV?
- No. PPG-based variability is related, but it is not identical to invasive arterial pulse pressure variation and can be affected by peripheral vascular tone.
- When does pleth variability work best?
- It works best in controlled mechanical ventilation with regular rhythm, stable tidal volumes, and clean signal conditions.
- Can it be used in spontaneously breathing patients?
- Its performance is weaker in spontaneous breathing because respiratory mechanics are less standardized and waveform variability is harder to interpret.
- Why do clinicians care about this metric?
- Because it may help identify fluid responsiveness without placing an arterial line, especially in perioperative or monitored acute care settings.