PPG Sensor: How It Works, LED Wavelengths, and Signal Formation Explained
How does a PPG sensor work? Learn LED light sources, photodetector basics, reflection vs transmission modes, and how blood volume changes create the PPG signal.
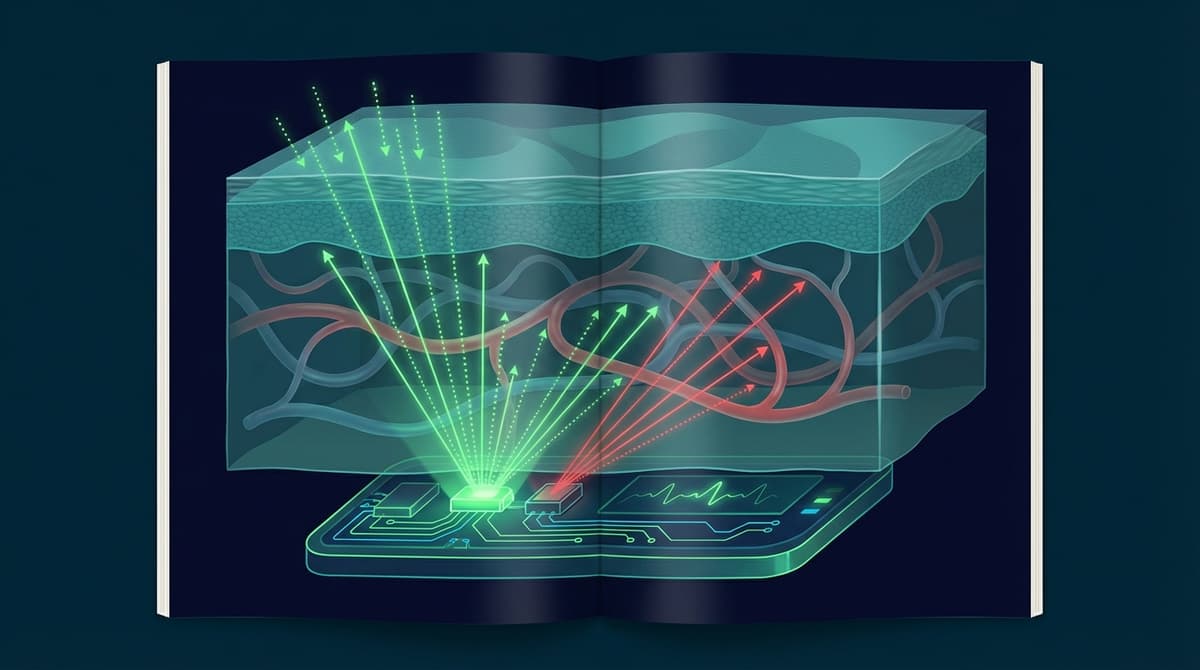
A PPG (photoplethysmography) sensor measures blood volume changes in the microvascular bed of tissue by shining light into the skin and detecting how much light is absorbed or reflected back. It consists of two core components: an LED light source and a photodetector. With each heartbeat, arterial blood flow increases in the capillaries, absorbing more light. The photodetector picks up this variation, producing a waveform that tracks your pulse in real time. This simple optical principle powers everything from hospital pulse oximeters to the heart rate monitor on your wrist.
The Two Core Components: LED and Photodetector
Every PPG sensor, regardless of form factor or application, boils down to the same two pieces of hardware.
LED Light Source
The LED emits light at a specific wavelength into the skin. Different wavelengths penetrate tissue to different depths and interact with hemoglobin differently. The choice of wavelength determines what the sensor can measure and how well it handles various skin tones and tissue types.
Most PPG sensors use one or more of the following:
-
Green LEDs (520-570 nm): The most common choice for wrist-based wearables. Green light has strong hemoglobin absorption, producing a high-amplitude pulsatile signal. It does not penetrate very deep, typically reaching only the superficial capillary beds. This makes green ideal for heart rate measurement but less useful for SpO2 estimation.
-
Red LEDs (620-660 nm): Red light penetrates deeper into tissue. It is used alongside infrared for blood oxygen saturation (SpO2) calculations because oxyhemoglobin and deoxyhemoglobin absorb red and infrared light at different ratios.
-
Infrared LEDs (850-950 nm): IR light penetrates the deepest and passes through tissue more easily than shorter wavelengths. Combined with red light, it enables pulse oximetry through the ratio-of-ratios method. IR is also less sensitive to skin pigmentation, making it important for accuracy across skin tones.
For a detailed breakdown of how wavelength selection affects measurement quality, see our PPG LED wavelength selection guide.
Photodetector
The photodetector sits near the LED and converts incoming light into an electrical signal. In most PPG sensor chips, this is a silicon photodiode with sensitivity tuned to match the LED wavelengths in use.
The photodetector must handle a wide dynamic range. The DC component of the optical signal (from tissue, bone, venous blood, and non-pulsatile arterial blood) is much larger than the AC pulsatile component you actually care about. The pulsatile portion might be only 1-5% of the total signal. This is why analog front-end design matters so much. The signal chain needs high-resolution ADCs and careful gain settings to resolve small pulsatile changes on top of a large baseline. Our overview of PPG photodetector technologies covers photodiode arrays, phototransistors, and CMOS sensor approaches in more detail.
Reflection Mode vs. Transmission Mode
PPG sensors operate in one of two optical configurations, and the choice has significant implications for where you can place the sensor and what signals you can capture.
Transmission Mode
In transmission mode, the LED and photodetector are on opposite sides of the tissue. Light passes through the tissue, and the detector picks up whatever makes it to the other side. This only works on thin body parts: fingertips, earlobes, or the toes of neonates.
Finger pulse oximeters use transmission mode. The clip holds the LED on one side of the finger and the photodetector on the other. Because the light travels through the full arterial bed, the signal tends to be strong and reliable. Transmission mode also handles motion artifacts reasonably well because the optical path is fixed by the clip.
Reflection Mode
In reflection mode, the LED and photodetector sit side by side on the same surface. Light enters the skin, scatters through tissue, and some of it bounces back to the detector. This configuration works on almost any body surface: the wrist, forehead, chest, or even the temple area inside an earbud.
The tradeoff is a weaker signal. Light scatters in all directions inside tissue, so only a fraction returns to the detector. The sensor is also more sensitive to contact pressure, skin surface conditions, and motion. However, reflection mode enables wearable PPG, which is why it dominates in smartwatches, fitness bands, and ring-form sensors.
For a direct comparison of both modes across clinical and consumer applications, see our reflection vs. transmission guide.
Signal Formation: AC and DC Components
The raw electrical output from a PPG photodetector is a composite signal with two distinct components that carry very different information.
DC Component (Baseline)
The DC component represents the overall light intensity reaching the detector after passing through (or reflecting from) tissue. It is determined by:
- Total tissue thickness and composition
- Venous blood volume
- Non-pulsatile arterial blood
- Bone, skin pigmentation, and muscle
- LED brightness and sensor-skin coupling
This baseline changes slowly with respiration (respiratory-induced intensity variation), body position, and temperature. It is relatively stable on a beat-to-beat timescale.
AC Component (Pulsatile)
The AC component is the small oscillation riding on top of the DC baseline. This oscillation is caused by the cardiac cycle. During systole, the left ventricle pushes blood into the arterial system. Arterioles in the capillary bed expand slightly, increasing the volume of blood in the optical path. More blood means more hemoglobin, which means more light absorption, which means less light reaches the photodetector.
During diastole, blood volume decreases, absorption drops, and more light reaches the detector.
The result is a periodic waveform synchronized with the heartbeat. The shape of this waveform contains information beyond just heart rate. The dicrotic notch (a small dip in the downslope) corresponds to aortic valve closure. The overall waveform morphology reflects arterial stiffness, vascular tone, and peripheral resistance.
The AC/DC ratio is what matters clinically. In pulse oximetry, the ratio of the AC component at red and infrared wavelengths (normalized by their respective DC values) directly determines blood oxygen saturation. This ratio-of-ratios approach eliminates the need to know absolute tissue properties.
What a PPG Sensor Actually Measures
It is worth being precise about this. A PPG sensor does not directly measure heart rate. It does not measure blood pressure. It does not measure blood oxygen.
What it measures is changes in blood volume in the tissue beneath the sensor. More specifically, it measures changes in the amount of light absorbed or reflected by that tissue over time. Because blood volume changes are driven by the cardiac cycle, you can extract heart rate from the signal. Because oxyhemoglobin and deoxyhemoglobin have different absorption spectra, you can estimate SpO2 using multi-wavelength measurements.
Everything else, including heart rate variability, respiration rate, blood pressure estimation, and stress metrics, is derived through algorithms applied to this fundamental blood-volume-change signal. The sensor provides the raw optical data. The intelligence lives in the signal processing pipeline. For a deeper look at the raw signal characteristics, see our PPG signal basics guide.
Common PPG Sensor Chips
Several integrated circuit manufacturers produce dedicated PPG analog front-end (AFE) chips that combine LEDs, photodetectors, ADCs, and ambient light cancellation into a single package. These chips handle the hardest parts of PPG signal acquisition so that device designers can focus on algorithms and product design.
Maxim MAX86150
The MAX86150 from Analog Devices (formerly Maxim Integrated) combines a PPG sensor and a single-lead ECG front end in one package. It includes three internal LEDs (red, IR, green), a photodetector, 19-bit ADC, and built-in ambient light cancellation. The combined PPG+ECG capability makes it popular in research platforms and clinical-grade wearables where both optical and electrical cardiac signals are needed.
Texas Instruments AFE4404
The AFE4404 is a flexible PPG analog front end that supports up to three LEDs and two photodiode inputs. It features a 22-bit ADC with programmable LED current control and timing. TI designed it for low-power wearable applications, and it appears in several commercial fitness devices. Its configurable architecture makes it a common choice for researchers building custom PPG sensors.
ams-OSRAM AS7050
The AS7050 (formerly AS7050 from ams) is optimized for wrist-worn and earbud-based heart rate monitoring. It includes a multi-channel optical readout, integrated LED drivers, and accelerometer interface for motion compensation. The chip handles much of the signal conditioning in hardware, reducing the processing burden on the host microcontroller. It supports up to eight photodiode channels, enabling sophisticated multi-wavelength measurements.
Other Notable Chips
- Analog Devices ADPD4101: High-channel-count optical AFE supporting up to 12 time slots for complex multi-wavelength configurations
- Silicon Labs Si117x: Ultra-low-power optical sensor family targeting always-on wearable applications
- Renesas OB1203: Combined PPG and proximity sensor for compact earbud and ring designs
Signal Processing: From Raw Photocurrent to Heart Rate
The raw signal coming out of a PPG photodetector is noisy and requires several processing stages before it yields useful physiological data.
Bandpass filtering removes frequencies outside the range of interest. For heart rate, a bandpass of roughly 0.5 to 4 Hz captures cardiac frequencies corresponding to 30-240 BPM while rejecting DC drift and high-frequency noise.
Motion artifact removal is often the biggest challenge. Accelerometer data from an IMU is used to identify and subtract motion-correlated components from the PPG signal. Adaptive filtering techniques like Normalized Least Mean Squares (NLMS) or Kalman filtering are common approaches.
Ambient light cancellation happens partly in hardware (the AFE chip subtracts ambient light samples taken between LED pulses) and partly in software. This is especially important for outdoor use where sunlight can saturate the photodetector.
Peak detection identifies individual pulse beats. Simple algorithms find local maxima in the filtered signal. More robust approaches use template matching, autocorrelation, or frequency-domain methods to handle noisy signals where individual peaks may be unclear.
Key Parameters That Affect Signal Quality
Several physical and physiological factors determine how clean a PPG signal you get from a given sensor configuration.
Contact pressure is surprisingly important in reflection mode. Too little pressure and the sensor does not couple well to the skin. Too much pressure and you occlude the capillary bed, flattening the pulsatile signal. Most wearable manufacturers specify a recommended wearing tightness for exactly this reason.
Skin pigmentation affects the DC baseline and can reduce the AC amplitude, particularly at green wavelengths. Higher melanin content absorbs more light before it reaches the vascular bed, leaving less light for the detector. IR wavelengths are less affected by melanin absorption, which is why multi-wavelength sensors perform better across diverse skin tones.
Hair and tattoos create optical barriers that block or scatter light before it reaches the capillary bed. Tattoo ink, especially dark ink, absorbs green light strongly and can reduce signal amplitude to unusable levels in the tattooed area.
Perfusion varies between individuals and with temperature. Cold extremities have reduced peripheral blood flow, resulting in a smaller pulsatile component. This is a common cause of poor signal quality in cold clinical environments or during outdoor winter exercise.
PPG vs. Other Optical Sensing Methods
PPG is one of several optical approaches used for physiological measurement, and it is worth understanding where it sits in relation to others.
Pulse oximetry is a specific application of PPG. All pulse oximeters are PPG sensors, but not all PPG sensors perform pulse oximetry. SpO2 measurement requires at least two wavelengths (red and IR) and calibration curves, while a basic PPG heart rate sensor can work with a single green LED.
Near-infrared spectroscopy (NIRS) uses similar optical principles but focuses on tissue oxygenation at greater depths. NIRS typically uses wavelengths in the 700-900 nm range and measures absolute or relative changes in oxygenated and deoxygenated hemoglobin concentration rather than pulsatile blood volume changes.
Remote PPG (rPPG) operates on the same blood-volume-change principle but uses a camera and ambient light instead of a dedicated LED and photodetector. The physics is identical, but the engineering challenges are very different. See our rPPG technology overview for details on the camera-based approach.
Frequently Asked Questions
What is a PPG sensor and how does it measure heart rate?
A PPG sensor uses an LED to shine light into the skin and a photodetector to measure how much light is absorbed or reflected. Blood volume changes with each heartbeat alter the amount of light reaching the detector, creating a pulsatile waveform. Heart rate is extracted by counting the peaks in this waveform or analyzing its frequency content.
Why do most smartwatches use green LEDs for PPG?
Green light (around 530-570 nm) has strong hemoglobin absorption, which produces a large pulsatile signal relative to the baseline. Green wavelengths also interact primarily with superficial capillary beds at the wrist, where the sensor sits. This combination gives a strong, reliable signal for heart rate measurement during daily activities. Red and IR LEDs are added when the device also needs to measure blood oxygen saturation.
What is the difference between reflection and transmission PPG?
In transmission mode, the LED and detector are on opposite sides of the tissue (like a finger clip). In reflection mode, they sit side by side on the same surface (like a smartwatch back). Transmission mode gives stronger signals but only works on thin body parts. Reflection mode works almost anywhere on the body but produces weaker signals and is more sensitive to motion and contact pressure.
Can PPG sensors work on all skin tones?
PPG sensors work across skin tones, but accuracy can vary. Higher melanin content absorbs more light, particularly at shorter (green) wavelengths, reducing the pulsatile signal amplitude. Modern sensors address this with adaptive LED brightness, multi-wavelength approaches, and infrared LEDs that are less affected by melanin. Research by Bent et al. (2020) documented accuracy differences across skin tones, published in npj Digital Medicine.
How accurate are PPG heart rate sensors compared to ECG?
Under resting conditions with good sensor contact, modern PPG sensors achieve mean absolute error (MAE) below 2 BPM compared to ECG reference. During moderate exercise, errors increase to 3-5 BPM due to motion artifacts. During high-intensity exercise, errors can exceed 10 BPM without advanced motion compensation. A validation study by Nelson and Allen (2019) provides detailed accuracy data in the Physiological Measurement journal.
What causes poor signal quality in PPG sensors?
The most common causes are motion artifacts (the sensor moves relative to the skin), poor contact pressure (too loose or too tight), low perfusion (cold skin, poor circulation), ambient light interference (bright sunlight overwhelming the detector), and optical barriers like dense body hair or dark tattoos over the sensor area.
What is the AC/DC ratio in PPG and why does it matter?
The AC component is the small pulsatile variation caused by each heartbeat. The DC component is the much larger baseline signal from tissue, venous blood, and non-pulsatile structures. The ratio between them, sometimes called the perfusion index, indicates how strong the cardiac signal is relative to the background. In pulse oximetry, the AC/DC ratios at red and IR wavelengths are used to calculate blood oxygen saturation.