Pulsus Bisferiens: Double-Peaked Pulse Waveform, Causes, and PPG Detection
What pulsus bisferiens is, how to identify the double-peaked arterial pulse, its causes (aortic regurgitation, HOCM), and detection via PPG waveforms.
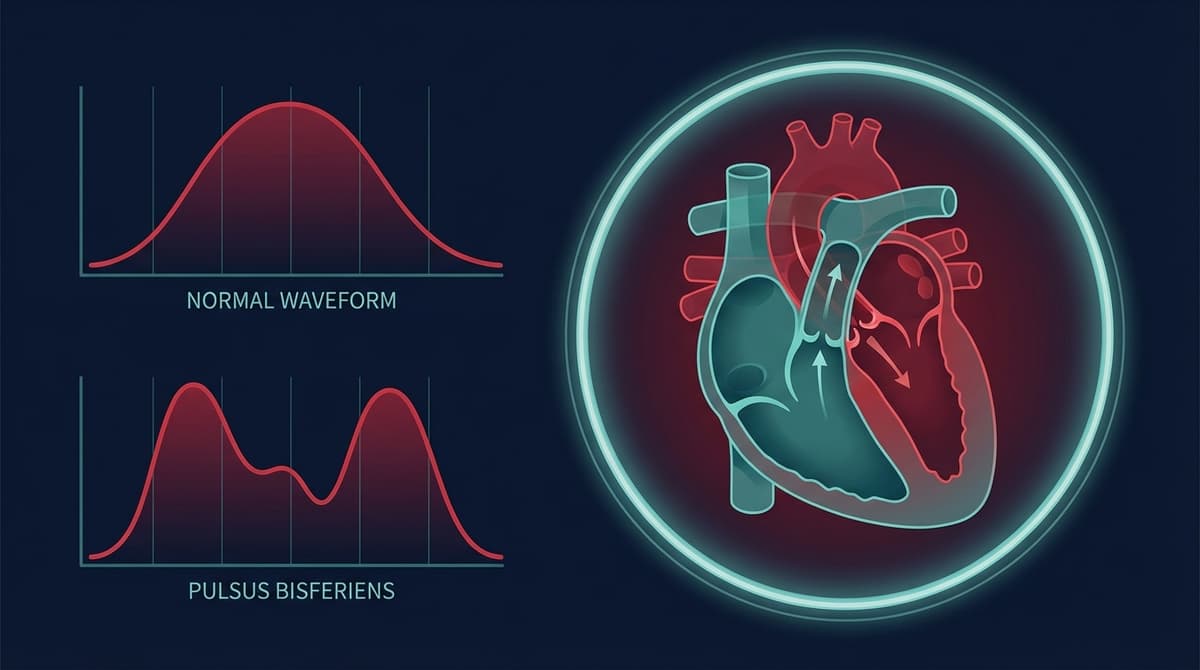
Pulsus bisferiens is an arterial pulse waveform characterized by two distinct systolic peaks separated by a mid-systolic dip, felt as a "double beat" on palpation or seen as a twin-peaked systolic contour on arterial line tracings. The name comes from the Latin "bis" (twice) and "feriens" (striking). It is most strongly associated with combined aortic stenosis and aortic regurgitation, hypertrophic obstructive cardiomyopathy (HOCM), and severe isolated aortic regurgitation. Recognizing this pattern on an arterial tracing, or potentially on a PPG waveform, points toward specific structural heart disease and can guide further diagnostic workup.
Unlike the normal dicrotic pulse (which has one systolic peak and one diastolic peak separated by the dicrotic notch), pulsus bisferiens shows two peaks that both occur during systole, before the dicrotic notch. This distinction is important because confusing the two patterns leads to entirely different clinical interpretations.
Pathophysiology: Why the Pulse Strikes Twice
The double-peaked systolic waveform results from specific hemodynamic conditions that create two distinct phases of forward flow during ventricular ejection.
In Aortic Regurgitation
Severe aortic regurgitation produces the classic bisferiens pulse through the following mechanism:
-
Large stroke volume. Because a significant volume of blood leaks back through the incompetent aortic valve during diastole, the left ventricle must eject a larger-than-normal stroke volume to maintain forward cardiac output. This volume overload dilates the ventricle and increases the force of contraction (Frank-Starling mechanism).
-
Rapid initial ejection (percussion wave). The large stroke volume is ejected forcefully into the aorta, creating a rapid initial pressure rise. The first peak, called the percussion wave, reflects this early, high-velocity ejection.
-
Mid-systolic pressure dip. As the initial bolus of blood moves distally and the rate of ejection slows, aortic pressure briefly falls. The Venturi effect from rapid blood flow past the aortic valve contributes to this mid-systolic drop.
-
Tidal wave (second peak). Reflected pressure waves returning from the periphery arrive during late systole and create the second peak, called the tidal wave. In normal physiology, reflected waves arrive during diastole. In aortic regurgitation, the wide pulse pressure and altered arterial hemodynamics cause reflected waves to arrive earlier, during systole.
When aortic stenosis coexists with regurgitation (mixed aortic valve disease), the bisferiens pattern is even more pronounced because the stenotic valve creates a midsystolic gradient that accentuates the dip between the percussion and tidal waves.
In Hypertrophic Obstructive Cardiomyopathy (HOCM)
The mechanism in HOCM is different and involves dynamic left ventricular outflow tract (LVOT) obstruction:
-
Rapid early ejection. The hypertrophied ventricle contracts forcefully, ejecting blood rapidly through the LVOT before obstruction develops. This produces the first peak, a brisk initial upstroke with a high peak.
-
Dynamic LVOT obstruction. As ejection progresses, the anterior mitral leaflet is pulled toward the interventricular septum by Venturi forces (systolic anterior motion, or SAM), progressively obstructing the outflow tract. This creates a mid-systolic drop in flow and pressure.
-
Late systolic secondary wave. The ongoing ventricular contraction against the obstruction generates a second pressure peak as blood continues to be forced through the narrowed LVOT. This late systolic rise may also incorporate reflected wave components.
The HOCM bisferiens pattern is sometimes described as "spike and dome": a sharp initial spike followed by a rounded dome. This shape is distinct from the aortic regurgitation pattern, which tends to show two peaks of more similar amplitude.
Identifying Pulsus Bisferiens on Arterial Line Tracings
On a calibrated arterial line waveform, pulsus bisferiens shows these characteristic features:
Two systolic peaks. Both peaks occur before the dicrotic notch. The first peak (percussion wave) and the second peak (tidal wave) are separated by a mid-systolic valley. The depth of the valley varies with severity: in mild cases, it may appear as a shoulder or flattening rather than a distinct dip.
Wide pulse pressure. In aortic regurgitation, pulse pressure is typically greater than 60 mmHg, often exceeding 80-100 mmHg. The diastolic pressure is low (often below 60 mmHg) due to regurgitant flow.
Rapid upstroke. The initial rise is steep, reflecting the forceful ejection against reduced afterload (in AR) or the vigorous early contraction (in HOCM).
Low diastolic pressure with rapid diastolic runoff. In AR, the incompetent aortic valve allows continuous backflow during diastole, producing a steep diastolic descent.
Position of the dicrotic notch. The dicrotic notch, marking aortic valve closure, follows the second systolic peak. Its position confirms that both peaks are systolic, not one systolic and one diastolic.
Differentiating Pulsus Bisferiens from Similar Waveform Patterns
Several pulse abnormalities can be confused with pulsus bisferiens. Correct differentiation requires attention to timing relative to the dicrotic notch.
Dicrotic Pulse
The dicrotic pulse shows an exaggerated diastolic wave following the dicrotic notch, creating what looks like a double peak. The difference: in the dicrotic pulse, the first peak is systolic and the second peak is diastolic (after the notch). In pulsus bisferiens, both peaks are systolic (before the notch). The dicrotic pulse occurs in low cardiac output states, sepsis, and severe heart failure, where reduced stroke volume and low peripheral resistance produce a prominent diastolic rebound. For more detail on the dicrotic notch and its physiological meaning, see our dicrotic notch physiology guide.
Pulsus Alternans
Pulsus alternans shows alternating strong and weak beats: one pulse has high amplitude, the next has lower amplitude, in a regular alternating pattern. Unlike bisferiens, this is a beat-to-beat variation, not a within-beat double peak. Pulsus alternans indicates severe left ventricular systolic dysfunction and is associated with advanced heart failure.
Normal Dicrotic Notch with Prominent Diastolic Peak
In young, healthy individuals with very compliant arteries, the dicrotic notch can be deep and the diastolic peak can be prominent, creating what appears to be a double peak on casual inspection. The timing is the key: the second hump follows the notch (diastolic) and is smaller than the systolic peak.
Pulsus Tardus et Parvus (Aortic Stenosis)
Severe aortic stenosis without regurgitation produces a slow-rising (tardus) and low-amplitude (parvus) pulse with a delayed systolic peak. There is no double peak. However, when stenosis and regurgitation coexist, the bisferiens pattern can appear.
Comparison summary:
| Pattern | Number of Peaks | Timing | Associated Conditions |
|---|---|---|---|
| Pulsus bisferiens | 2 systolic peaks (before notch) | Both systolic | AR, HOCM, mixed aortic disease |
| Dicrotic pulse | 1 systolic + 1 diastolic (after notch) | Systolic then diastolic | Low output, sepsis |
| Pulsus alternans | Alternating strong/weak beats | Beat-to-beat | Severe LV failure |
| Normal dicrotic notch | 1 systolic + visible notch + small diastolic hump | Standard | Young, healthy |
PPG Detection of Pulsus Bisferiens
Can photoplethysmography detect pulsus bisferiens? The answer is conditional: yes in some cases, with important caveats.
What PPG Can Show
PPG waveforms from finger pulse oximeters have demonstrated double-peaked systolic contours in patients with confirmed bisferiens patterns on simultaneous arterial line tracings. Several case reports and small studies have documented PPG-visible bisferiens:
- Foo et al. (2005) demonstrated that finger PPG waveform morphology in patients with aortic regurgitation showed clear double systolic peaks corresponding to bisferiens patterns on simultaneous radial artery tonometry.
- Shin and Kim (2017) used smartphone-based PPG to identify abnormal pulse contours including bisferiens-like patterns, though sensitivity was limited compared to clinical palpation (DOI: 10.1038/s41598-017-14891-0).
The bisferiens pattern is most visible in finger PPG, where the arterial signal is strongest and the waveform morphology is best preserved. Wrist PPG from smartwatches typically lacks sufficient waveform fidelity to resolve the mid-systolic dip.
Challenges for PPG-Based Detection
Signal quality. The mid-systolic dip in pulsus bisferiens can be subtle, on the order of a few percent of the pulse amplitude. Motion artifacts, baseline wander, and low perfusion can easily obscure this feature.
Peripheral amplification. PPG measures volumetric changes in peripheral arterioles, not direct arterial pressure. The peripheral vascular bed acts as a low-pass filter that smooths high-frequency features of the central waveform. This can attenuate the valley between the two systolic peaks.
Sampling rate. Detecting a brief mid-systolic dip requires adequate temporal resolution. Consumer PPG sensors with sampling rates of 25-50 Hz may not resolve the feature, while clinical PPG at 250-1000 Hz provides sufficient temporal detail.
Absence of reference values. No validated algorithm or threshold exists for automatically classifying a PPG waveform as bisferiens versus normal with a prominent reflected wave component. The distinction requires contextual interpretation.
Toward Automated Detection
Machine learning approaches to PPG waveform classification have shown promise for detecting abnormal pulse contours. Convolutional neural networks trained on labeled PPG waveforms can identify patterns like bisferiens, pulsus alternans, and irregular rhythms with sensitivities of 80-90% in controlled research settings. However, these systems have not been validated for clinical use in detecting specific valvular lesions.
The more realistic near-term application is flagging: a wearable PPG device that detects persistently abnormal pulse contours could alert the user to seek medical evaluation, rather than attempting a specific diagnosis. For background on how the cardiac cycle maps onto the PPG waveform, see our cardiac cycle phases in PPG guide.
Clinical Significance and Associated Conditions
Pulsus bisferiens is not common, but when present, it points toward a short list of serious conditions:
Severe aortic regurgitation (chronic). This is the most common cause. Chronic AR allows the left ventricle to adapt through dilation and increased compliance, producing the large stroke volume needed to generate the bisferiens pattern. Acute severe AR (from endocarditis or aortic dissection) typically does not produce bisferiens because the ventricle has not had time to dilate.
Combined aortic stenosis and regurgitation. Mixed aortic valve disease produces the most classic and pronounced bisferiens pattern. The stenosis creates turbulent flow and the regurgitation provides the volume overload.
Hypertrophic obstructive cardiomyopathy. The bisferiens pattern in HOCM has the characteristic spike-and-dome morphology. Its presence on physical examination is considered a supporting sign for dynamic LVOT obstruction, though echocardiography is required for definitive diagnosis.
High-output states (rare). Severe anemia, thyrotoxicosis, large arteriovenous fistulae, and other causes of high cardiac output can occasionally produce a bisferiens-like pattern due to the combination of large stroke volume and low peripheral resistance.
Patent ductus arteriosus (PDA). In neonates with large PDAs, the diastolic run-off into the pulmonary circulation widens the pulse pressure and can produce a bisferiens contour.
Pulsus Bisferiens on Physical Examination
Detecting pulsus bisferiens by palpation is a classic bedside skill but one that requires practice. The double beat is best felt at the carotid artery, where the waveform is closest to the central aortic pulse. At the radial artery, the two peaks may be less distinct due to peripheral filtering.
Technique for carotid palpation:
- Use gentle pressure with the index and middle fingers over the carotid artery, just lateral to the thyroid cartilage.
- Avoid compressing the artery, as this distorts the waveform.
- Feel for two distinct impulses per heartbeat, separated by a brief softening.
- Compare with the opposite carotid.
In clinical practice, pulsus bisferiens is detected by palpation in fewer than 50% of cases where it is visible on arterial line tracings. This low sensitivity is why invasive monitoring and increasingly PPG-based waveform analysis have value: they detect what the fingertip misses.
For an overview of how invasive arterial waveforms compare to non-invasive PPG, see our PPG waveform basics guide. Additional context on how arterial stiffness shapes the PPG waveform is available in our PPG aortic stiffness biomarker analysis.
Frequently Asked Questions
What does pulsus bisferiens feel like on palpation?
Pulsus bisferiens feels like two quick taps per heartbeat at the carotid pulse, sometimes described as a "double flick." The two impulses happen close together during systole, separated by a brief softening. It is most easily felt at the carotid artery and may not be detectable at the radial artery. In practice, most clinicians find it difficult to identify reliably by palpation alone.
What is the difference between pulsus bisferiens and a dicrotic pulse?
In pulsus bisferiens, both peaks occur during systole, before the dicrotic notch. In a dicrotic pulse, the first peak is systolic and the second is diastolic, after the dicrotic notch. Bisferiens indicates structural heart disease (aortic regurgitation, HOCM), while a dicrotic pulse is seen in low cardiac output states like sepsis or severe heart failure.
What causes pulsus bisferiens?
The most common causes are combined aortic stenosis and aortic regurgitation, severe isolated aortic regurgitation, and hypertrophic obstructive cardiomyopathy (HOCM). In AR, the mechanism involves large stroke volume with early and late systolic pressure peaks. In HOCM, dynamic outflow tract obstruction creates a mid-systolic drop between an early spike and a late dome.
Can a smartwatch PPG detect pulsus bisferiens?
Current smartwatch PPG sensors generally lack the waveform fidelity needed to resolve the subtle mid-systolic dip that defines bisferiens. Finger-based PPG with clinical-grade sensors and high sampling rates (250+ Hz) can detect the pattern in some patients. Wrist PPG may eventually achieve this with improved sensor technology and signal processing.
Is pulsus bisferiens dangerous?
Pulsus bisferiens itself is a physical sign, not a disease. However, the conditions that cause it, severe aortic regurgitation, HOCM with obstruction, and mixed aortic valve disease, are serious and often require surgical intervention. The presence of bisferiens should prompt echocardiographic evaluation and cardiology referral.
How is pulsus bisferiens different from pulsus alternans?
Pulsus alternans shows alternating strong and weak beats in a regular pattern (every other beat is weaker). Pulsus bisferiens shows two peaks within a single beat. Alternans indicates severe left ventricular dysfunction, while bisferiens points toward valvular or outflow tract obstruction disease.
Can pulsus bisferiens go away?
In aortic regurgitation, the bisferiens pattern may resolve if the valve is repaired or replaced (surgically or with TAVR). In HOCM, the pattern may decrease with medical treatment (beta-blockers, disopyramide) that reduces the dynamic outflow gradient, or after septal myectomy or alcohol septal ablation. If the underlying cause is corrected, the waveform normalizes.