PPG Orthostatic Hypotension Detection: Can Optical Pulse Signals Catch a Standing BP Drop?
PPG orthostatic hypotension detection uses beat-to-beat pulse changes to flag standing blood pressure drops, offering screening value but not a cuffless diagnosis.
PPG orthostatic hypotension detection uses optical pulse wave changes during a posture transition to flag a possible standing blood pressure drop. It can be surprisingly informative because standing alters stroke volume, vascular tone, and heart rate within seconds, but PPG should be treated as a screening tool, not a formal replacement for cuff or beat-to-beat blood pressure measurement.
Definition box: Orthostatic hypotension is a sustained drop in blood pressure after standing, commonly defined as at least 20 mmHg systolic or 10 mmHg diastolic within 3 minutes.
This topic matters because orthostatic symptoms are common and often under-captured. Patients say they feel dizzy when they stand up, but by the time they sit in clinic the moment has passed. A wearable, especially one that captures transitions in daily life, can help surface a pattern that deserves formal testing.
Can a PPG signal really reflect a standing blood pressure drop?
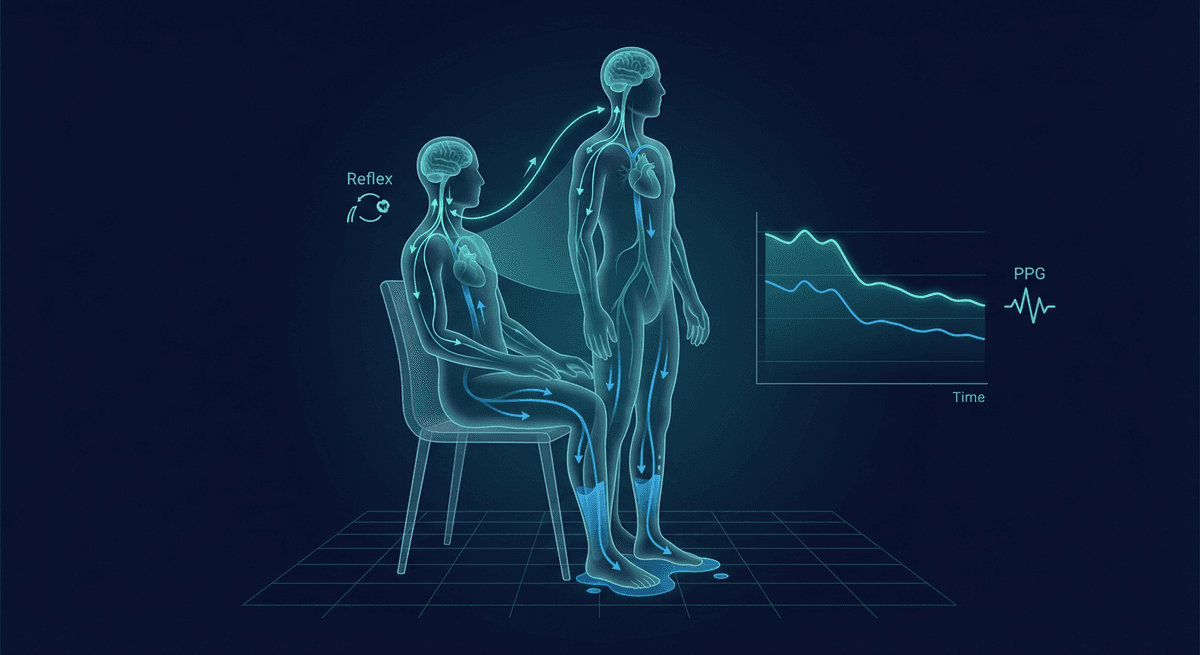
Yes, indirectly. PPG is not measuring pressure in mmHg. It is measuring the peripheral pulse wave. When someone stands up, gravity shifts blood volume downward, venous return falls, stroke volume drops, and the body compensates through autonomic reflexes.
That sequence changes the optical pulse in several ways:
- pulse amplitude often falls initially
- inter-beat intervals shorten as heart rate rises
- systolic upstroke characteristics can shift
- peripheral vasoconstriction modifies waveform shape
- recovery time reveals autonomic competence
Those dynamics make PPG useful for posture-change screening.
For background physiology, PPG baroreceptor reflex autonomic and PPG autonomic function testing are useful companion reads.
What does the waveform do when a person stands?
The first 15 to 30 seconds after standing are often the most revealing.
Immediate phase
Venous pooling reduces preload. Stroke volume falls. The peripheral pulse may shrink quickly, and beat intervals shorten as compensatory tachycardia starts.
Recovery phase
If autonomic reflexes are intact, vascular tone increases and pressure recovers. The pulse waveform partially stabilizes.
Impaired recovery
In autonomic dysfunction, dehydration, medication-related hypotension, or frailty, the amplitude drop may be larger, recovery slower, and symptoms more likely.
This is why timing matters. A wearable that only averages over minutes can miss the most interesting part.
Which PPG features are useful for orthostatic detection?
Several feature families matter.
Pulse amplitude change
A drop in amplitude after standing is common. The exact size varies by sensor site and person, but relative change can be informative.
Heart rate response
The inter-beat interval shortens with standing. Excessive tachycardia may point toward orthostatic intolerance or POTS rather than classic orthostatic hypotension.
Recovery slope
How quickly the pulse waveform stabilizes can reflect autonomic compensation.
Morphology features
Systolic rise time, notch visibility, and pulse width may shift as vascular tone changes. These are not perfect direct surrogates for blood pressure, but they add context.
Contextual signals
Accelerometer data confirms the posture transition. Without that, PPG features alone are harder to interpret.
Where PPG helps most in clinical practice
Screening outside the lab
Formal orthostatic vitals are useful, but they capture a narrow window. Wearables can catch repeated episodes at home, especially in people who experience symptoms during daily routines.
Older adults with falls or near-syncope
Orthostatic blood pressure recovery is linked to fall risk. A wearable may not diagnose the problem, but it can identify a repeated abnormal transition worth escalating.
Autonomic dysfunction populations
Patients with Parkinsonian disorders, diabetic neuropathy, long COVID, or medication effects often have posture-related symptoms that fluctuate day to day.
Therapy monitoring
If a clinician changes hydration strategy, compression therapy, salt intake, or medication timing, a wearable may provide trend-level feedback on whether posture tolerance improved.
Where PPG falls short
This is the key limitation: PPG does not output validated standing blood pressure in a way that replaces orthostatic vitals.
Problems include:
- sensor-specific amplitude behavior
- sensitivity to peripheral vasoconstriction
- motion during the stand itself
- weak wrist perfusion in symptomatic patients
- person-to-person calibration differences
A clean-looking pulse drop is suggestive, not diagnostic.
That is why PPG-based orthostatic screening sits closer to PPG continuous blood pressure research than to routine clinical BP replacement.
Orthostatic hypotension versus POTS: why the distinction matters
These conditions are often mixed together online, but they are not the same.
Orthostatic hypotension
The defining issue is a blood pressure drop after standing.
POTS
The defining issue is an excessive heart rate rise on standing without the same sustained BP drop pattern.
PPG can help show both amplitude changes and heart rate response, which makes it useful for screening. Still, proper diagnosis needs standardized criteria and formal measurements.
Practical study design for wearable orthostatic monitoring
If you were building a protocol, you would want:
- supine rest baseline
- clear timestamp of stand initiation
- beat-to-beat pulse detection for at least 3 minutes
- simultaneous accelerometer confirmation
- symptom tagging
- if possible, paired cuff or continuous BP ground truth
Without good timing, the physiology gets blurred.
Best real-world use case right now
The best use case is not replacing formal orthostatic vitals. It is triage.
If someone has repeated dizziness on standing, a wearable that consistently shows abrupt pulse amplitude loss, strong compensatory tachycardia, and poor recovery gives the clinician a more concrete reason to test further.
That is valuable, especially in telehealth and home monitoring settings.
FAQ
Can PPG detect orthostatic hypotension?
PPG can detect pulse waveform changes that often accompany orthostatic hypotension, so it works as a screening tool, but it does not replace formal blood pressure measurement.
What happens to the PPG signal when someone stands up?
Standing changes venous return, stroke volume, pulse amplitude, and heart rate, which together can reshape the PPG waveform over the first seconds after standing.
Is PPG useful for autonomic dysfunction screening?
Yes. PPG can help screen for autonomic dysfunction because posture change responses are reflected in pulse timing, amplitude, and recovery dynamics.
Can a smartwatch diagnose POTS or orthostatic hypotension?
No. A smartwatch may support suspicion, but diagnosis still requires standardized clinical criteria and proper blood pressure and heart rate measurements.
Who might benefit from PPG-based orthostatic monitoring?
People with dizziness, syncope, neuropathy, Parkinsonian disorders, long COVID, dehydration, or medication-related hypotension may benefit from structured screening.
How to validate a wearable orthostatic algorithm
A solid validation study needs more than symptom reports. The best design pairs PPG with continuous beat-to-beat blood pressure or at least tightly timed cuff measurements during a standardized active stand or tilt-table test.
Important protocol elements include:
- several minutes of quiet supine baseline
- exact timestamp of standing or tilt change
- continuous recording through the first 3 minutes
- repeat tests on separate days to assess reproducibility
- subgroup analysis for age, medication use, neuropathy, and arrhythmia
Without that structure, a model may look impressive in a small dataset and then fail in real use.
Sensor site matters more than many people expect
A finger or ear site may show clearer pulse amplitude changes than the wrist because the pulsatile signal is stronger. The wrist is easier for day-to-day wear, but it is a harder measurement site for fine hemodynamic interpretation. That trade-off sits at the heart of many wearable BP problems.
Frequently Asked Questions
- Can PPG detect orthostatic hypotension?
- PPG can detect pulse waveform changes that often accompany orthostatic hypotension, so it works as a screening tool, but it does not replace formal blood pressure measurement.
- What happens to the PPG signal when someone stands up?
- Standing changes venous return, stroke volume, pulse amplitude, and heart rate, which together can reshape the PPG waveform over the first seconds after standing.
- Is PPG useful for autonomic dysfunction screening?
- Yes. PPG can help screen for autonomic dysfunction because posture change responses are reflected in pulse timing, amplitude, and recovery dynamics.
- Can a smartwatch diagnose POTS or orthostatic hypotension?
- No. A smartwatch may support suspicion, but diagnosis still requires standardized clinical criteria and proper blood pressure and heart rate measurements.
- Who might benefit from PPG-based orthostatic monitoring?
- People with dizziness, syncope, neuropathy, Parkinsonian disorders, long COVID, dehydration, or medication-related hypotension may benefit from structured screening.