PPG Hypertension Cuffless Monitoring
Hypertension affects 1.28 billion adults worldwide and is the leading modifiable risk factor for cardiovascular disease. The standard cuff sphygmomano...
Hypertension affects 1.28 billion adults worldwide and is the leading modifiable risk factor for cardiovascular disease. The standard cuff sphygmomanometer, invented in the 1880s, is still the clinical gold standard. PPG-based cuffless blood pressure monitoring promises to change this, enabling continuous BP monitoring from a wrist device without the inconvenience of inflation. The promise is real; the technical and regulatory hurdles are substantial.
Why Cuffless BP Monitoring Is Difficult
Traditional cuff-based measurement works by occluding the brachial artery and listening or sensing for Korotkoff sounds as the cuff deflates. It is a direct measurement of arterial occlusion pressure.
PPG-based methods are indirect. They infer blood pressure from features of the arterial pulse waveform or from the time it takes the pulse to travel between two points. Neither method has a simple, stable, linear relationship with blood pressure across all people and conditions, which is the core technical challenge.
Blood pressure changes second-to-second with posture, emotion, activity, and vasoconstriction. The cuff captures a snapshot; PPG-based methods promise continuous tracking but must account for all these confounding sources of physiological variation.
The Three Main Technical Approaches
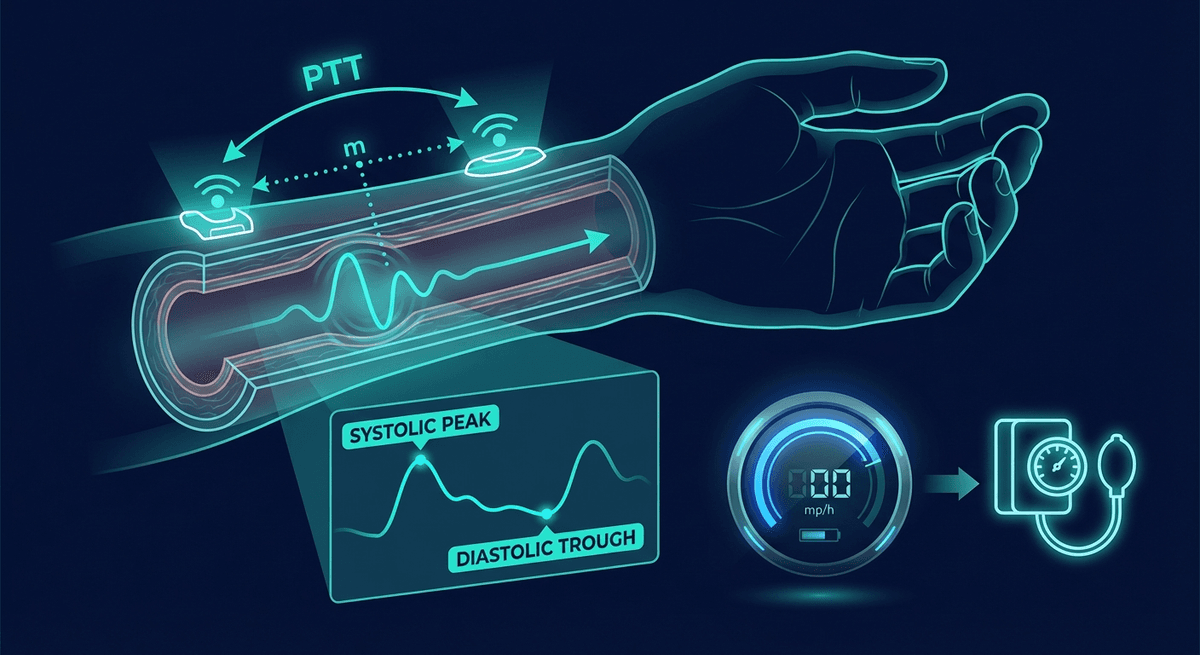
1. Pulse Transit Time (PTT)
PTT is the time for the arterial pulse wave to travel from the heart to a peripheral site. Because stiffer vessels transmit the wave faster, and because blood pressure increases vessel stiffness via the Frank-Starling mechanism, PTT inversely correlates with blood pressure: shorter PTT corresponds to higher BP.
To measure PTT, you need two sensors: a proximal timing reference (usually ECG R-wave or a PPG sensor at the ear, chest, or finger) and a distal PPG sensor (wrist or finger). The time difference is PTT.
Limitations:
- PTT varies with pre-ejection period and autonomic state, not just blood pressure
- The relationship is nonlinear and highly individual (requires personal calibration)
- Small timing differences (10–30 ms for a 10 mmHg change) require precise synchronization
- Recalibration is needed after changes in arterial stiffness from exercise, hydration, or position
Several research devices have demonstrated PTT-based BP estimation within 5–8 mmHg mean absolute error after personal calibration, which approaches the AAMI standard for clinical validation (mean error <5 mmHg, standard deviation <8 mmHg).
2. Pulse Wave Analysis (PWA)
Rather than measuring transit time, PWA extracts morphological features from the PPG waveform itself: systolic upstroke slope, peak amplitude, dicrotic notch position, diastolic decay rate, and augmentation index. These features reflect the interaction of cardiac output with arterial compliance and peripheral resistance, which collectively determine blood pressure.
Machine learning models (particularly neural networks trained on large paired datasets of PPG waveforms with simultaneous cuff BP) can learn the mapping from waveform features to blood pressure values. This approach does not require a second sensor but is highly dependent on the quality and diversity of the training data.
The challenge: the same PPG waveform can be produced by different combinations of cardiac output, compliance, and vascular resistance. This degeneracy means the mapping from waveform to BP is fundamentally underdetermined without additional physiological context.
3. Oscillometric PPG Methods
Some devices combine cuff inflation with PPG sensing instead of Korotkoff sounds, using the oscillations in PPG amplitude during cuff deflation to determine systolic and diastolic pressure more precisely. This is still a cuff-based measurement but potentially more accurate than traditional auscultation methods.
This approach does not provide continuous monitoring but may improve accuracy for discrete measurements. It is used in some clinical-grade devices.
Validation Studies and Current Accuracy
The IEEE Standard for Wearable, Cuffless Blood Pressure Measuring Devices (IEEE 1708-2014) and the Association for the Advancement of Medical Instrumentation (AAMI) SP10 standard set the accuracy bar: mean error <5 mmHg, standard deviation <8 mmHg, measured against a calibrated reference.
Current consumer devices generally do not meet these standards for uncalibrated BP estimation. A systematic review by Solà and Delgado-Gonzalo (2019, doi:10.3390/s19112353) evaluated studies of cuffless BP measurement and found:
- PTT-based methods after personal calibration: mean absolute error 5–10 mmHg (close to, but not consistently meeting, clinical standards)
- PWA-based methods from wrist PPG: mean absolute error 8–15 mmHg (acceptable for trend monitoring, not clinical diagnosis)
- ML-based methods on large training sets: mean absolute error 4–7 mmHg in the test dataset, with performance declining for out-of-distribution subjects
The Samsung Galaxy Watch 4 and 5 received CE mark approval in several countries for blood pressure monitoring using a pulse wave analysis approach combined with initial calibration against a cuff device. Samsung's published validation data showed mean systolic BP error of 1.6 mmHg and mean diastolic error of 1.2 mmHg after calibration, with standard deviations of approximately 7.5 mmHg. This meets AAMI criteria after calibration, but calibration drift over time remains a practical limitation.
The Recalibration Problem
Every PPG-based BP method that achieves clinical-grade accuracy requires personal calibration: a cuff measurement that anchors the individual's personal PTT-to-BP or waveform-to-BP relationship. The problem is that this relationship changes:
- After aerobic exercise, arteries dilate and become more compliant, shifting the calibration
- After caffeine, vasoconstriction shifts the baseline
- With posture changes (standing vs. lying), hydrostatic pressure shifts diastolic BP
- Over days to weeks, changes in cardiovascular fitness or medication effects alter the relationship
Samsung recommends recalibration every 4 weeks. Research suggests this may be insufficient for hypertensive patients where treatment titration depends on accurate absolute values. For trend monitoring in normotensive individuals, less frequent recalibration may be acceptable.
Regulatory Status
As of early 2026, the landscape is:
FDA (United States): No PPG-based consumer device has received FDA clearance for blood pressure monitoring. The FDA has issued guidance indicating that it will evaluate these devices under Class II (De Novo or 510(k)) pathway but has set strict validation requirements. Samsung does not market its Galaxy Watch BP feature in the United States.
CE Mark (Europe): Samsung Galaxy Watch 4/5/6 received CE mark for BP monitoring. Withings ScanWatch 2 received CE mark with BP monitoring via POWR (Pulse Wave Recording) technology.
South Korea: Samsung's BP monitoring feature received regulatory approval and has been available longer than in other markets.
The regulatory divergence between the US and Europe means US users cannot access some BP features available on the same hardware in European markets.
Clinical Implications for Hypertension Management
Despite the accuracy limitations, PPG-based BP monitoring shows genuine clinical potential for specific applications:
White coat hypertension detection: A patient who measures normal on a 24-hour ambulatory BP monitor but high in the clinic has white coat hypertension, which requires different management than true hypertension. PPG-based continuous monitoring could potentially replace some ambulatory BP monitoring indications.
Nocturnal hypertension: BP normally dips 10–20% during sleep. Non-dippers and reverse dippers have significantly higher cardiovascular risk. Detecting nocturnal BP patterns with a wearable is clinically meaningful, even with calibration-dependent accuracy.
BP variability assessment: Moment-to-moment and day-to-day BP variability is an independent cardiovascular risk factor, distinct from average BP. PPG-based continuous monitoring, even with absolute accuracy limitations, can characterize variability patterns that a clinic measurement cannot.
What Consumers Should Know
Currently available consumer BP features on smartwatches are best used for trend monitoring, not absolute measurement. The numbers should not be used to:
- Self-diagnose hypertension
- Adjust or stop antihypertensive medications
- Replace clinic measurements for treatment decisions
They can appropriately be used for:
- Noticing that BP is trending higher over weeks and prompting a clinic visit
- Understanding patterns throughout the day (activity, stress, sleep effects)
- Motivating lifestyle modifications with real-time feedback
For clinical BP management, a validated upper-arm cuff device remains the appropriate tool.
Internal Links
- For the technical details of PTT-based BP estimation: PPG Pulse Transit Time Blood Pressure
- For waveform analysis techniques: PPG Waveform Decomposition
- For continuous BP in ICU settings: PPG vs ABP Comparison
FAQ
Can a smartwatch accurately measure blood pressure? Current smartwatches that offer BP estimation (Samsung Galaxy Watch in many markets, some Withings devices) use PPG waveform analysis with personal calibration. After calibration, they can track blood pressure trends reasonably well, but their absolute accuracy does not consistently meet clinical standards without frequent recalibration. They should not replace validated upper-arm cuff devices for clinical decisions.
What is the most accurate wearable blood pressure monitor? Validated upper-arm cuff devices remain most accurate. Among PPG-based wearable devices, Samsung Galaxy Watch with calibration has published validation data meeting AAMI criteria. Withings ScanWatch 2 and some emerging devices also show promise. No wrist-worn PPG device consistently outperforms a calibrated upper-arm cuff.
How does pulse transit time measure blood pressure? The pulse wave generated by each heartbeat travels through the arteries at a speed that depends on vessel stiffness, which is related to blood pressure. Stiffer (higher-pressure) vessels transmit the wave faster, resulting in a shorter pulse transit time. By measuring how long the pulse takes to travel from the heart to the wrist, BP can be estimated, but this requires personal calibration.
Why is cuffless blood pressure monitoring not FDA-approved yet? The FDA requires rigorous clinical validation meeting specific accuracy standards before clearing devices for blood pressure monitoring claims. Current PPG-based devices, particularly those requiring calibration or showing accuracy that degrades over time, have not consistently met these standards. The FDA has issued guidance on what validation studies are needed.
Is continuous blood pressure monitoring useful for hypertension management? Potentially yes, for specific indications: detecting white coat hypertension, characterizing nocturnal BP patterns, and monitoring BP variability. However, absolute accuracy limitations mean current consumer devices are not appropriate for clinical decision-making without parallel cuff-based confirmation.
How often should I recalibrate my smartwatch blood pressure monitor? Samsung recommends monthly recalibration. Research suggests more frequent recalibration (weekly) may be needed after significant lifestyle changes (starting exercise, changing diet, new medications). After any major physiological change, recalibrate before relying on the readings.
Frequently Asked Questions
- Can a smartwatch accurately measure blood pressure?
- Current smartwatches with BP estimation use PPG waveform analysis with personal calibration. After calibration, they track trends reasonably well, but do not consistently meet clinical accuracy standards. They should not replace validated upper-arm cuff devices for clinical decisions.
- How does pulse transit time measure blood pressure?
- The pulse wave travels through arteries at a speed related to vessel stiffness, which increases with blood pressure. Shorter pulse transit time corresponds to higher blood pressure. Measurement requires personal calibration to account for individual arterial characteristics.
- Why is cuffless blood pressure monitoring not FDA-approved yet?
- The FDA requires rigorous clinical validation meeting specific accuracy standards. Current PPG-based devices have not consistently met these standards, particularly regarding accuracy stability over time without frequent recalibration.