Arterial Line Waveform Interpretation: Normal Anatomy, Damping, and PPG Comparison
How to read arterial line waveforms. Covers normal waveform anatomy, overdamping, underdamping, square wave test, artifacts, and PPG waveform comparison.
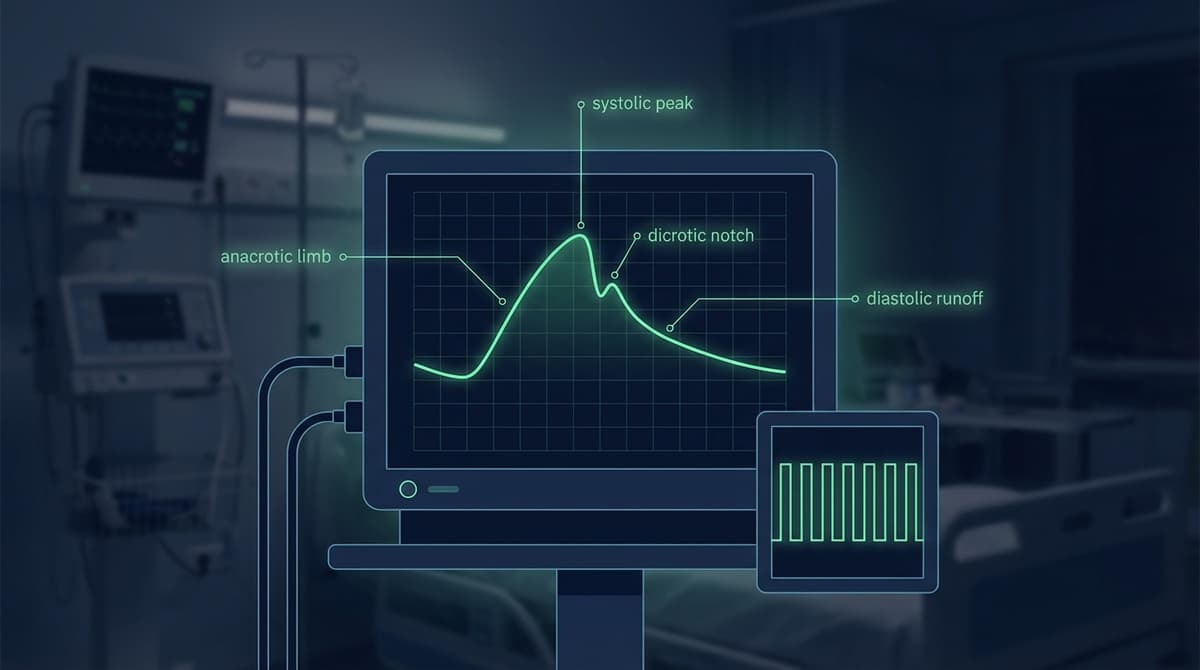
An arterial line waveform is the continuous pressure tracing produced by an indwelling arterial catheter connected to a fluid-filled transducer system. The normal waveform has a sharp systolic upstroke (anacrotic limb), a well-defined systolic peak, a clear dicrotic notch on the descending limb, and a gradual diastolic runoff that falls to the end-diastolic pressure before the next beat. Reading this waveform correctly provides real-time information about systolic pressure, diastolic pressure, mean arterial pressure, stroke volume, and vascular tone. When the waveform is distorted by overdamping or underdamping, the numerical values displayed on the monitor become unreliable, and the clinical team must identify and correct the source of distortion before acting on the readings.
Understanding arterial line waveforms also provides a reference frame for interpreting PPG signals, which capture many of the same hemodynamic features through a non-invasive optical method. The relationship between these two waveform types is a growing area of interest as PPG-based monitoring expands from pulse oximetry into blood pressure estimation and cardiac output trending.
Normal Arterial Waveform Anatomy
Each cardiac cycle produces a characteristic arterial pressure waveform with distinct phases that correspond to specific mechanical events.
The Anacrotic Limb (Systolic Upstroke)
The anacrotic limb is the steep rising edge at the beginning of systole. It starts when the aortic valve opens and the left ventricle begins ejecting blood into the aorta. The rate of rise (dP/dt) reflects the force and speed of ventricular contraction, the compliance of the proximal aorta, and the afterload against which the ventricle is ejecting.
A normal anacrotic limb rises sharply and smoothly. A slow, slurred upstroke (pulsus tardus) suggests aortic stenosis, where the narrowed valve restricts the flow rate. An unusually steep, brisk upstroke may indicate high cardiac output states, aortic regurgitation, or reduced proximal aortic compliance (increased stiffness).
The anacrotic notch (or anacrotic shoulder) is a small inflection sometimes visible partway up the rising limb. It represents the transition from the rapid ejection phase to the reduced ejection phase and is more prominent in central aortic tracings than in peripheral arterial lines.
The Systolic Peak
The systolic peak marks the highest pressure reached during ventricular ejection. In a radial arterial line, the systolic peak is typically 5-15 mmHg higher than in the central aorta due to peripheral amplification, the phenomenon by which pulse pressure increases as the wave travels distally through narrowing, stiffer arteries. This is a normal physiological effect, not an artifact.
Systolic peak pressure in healthy adults ranges from 100-140 mmHg. The height of the peak depends on stroke volume, heart rate, arterial compliance, and peripheral vascular resistance.
The Dicrotic Notch
The dicrotic notch is the small, sharp downward deflection on the descending limb of the waveform. It corresponds to aortic valve closure: when left ventricular pressure falls below aortic pressure, the aortic valve snaps shut, creating a brief pressure transient.
In central aortic tracings, this is called the incisura and appears as a sharp V-shaped notch. In peripheral arterial lines, the incisura is smoothed into the dicrotic notch due to wave reflection and damping in the arterial tree.
The dicrotic notch provides clinical information:
- Position on the waveform: A high-positioned notch (appearing high on the descending limb) suggests high peripheral vascular resistance. A low-positioned notch (near the diastolic nadir) suggests low peripheral resistance.
- Depth: A deep, well-defined notch indicates good aortic valve competence and adequate arterial compliance. A shallow or absent notch may indicate aortic regurgitation (valve fails to close properly) or reduced arterial compliance.
- Absence: Complete absence of the dicrotic notch raises concern for aortic regurgitation or severe arterial stiffness. It can also indicate overdamping in the monitoring system.
For a detailed analysis of the dicrotic notch and its clinical significance, see our PPG dicrotic notch physiology guide.
Diastolic Runoff
After the dicrotic notch, pressure declines exponentially as blood runs off from the elastic arterial system into the capillary bed. The rate of diastolic decline reflects total peripheral resistance and arterial compliance (the Windkessel function). A steep diastolic decline (low diastolic pressure) suggests low peripheral resistance (vasodilation, sepsis) or aortic regurgitation. A gradual decline (well-maintained diastolic pressure) suggests adequate peripheral vascular tone.
End-Diastolic Pressure
The lowest pressure reached just before the next systolic upstroke is the diastolic blood pressure. In the radial artery, diastolic pressure is usually 2-5 mmHg lower than central aortic diastolic pressure.
The Damping Problem: Too Much, Too Little, Just Right
The arterial line monitoring system consists of an arterial catheter, fluid-filled tubing, stopcocks, a flush device, and a pressure transducer. This system has its own mechanical properties, specifically natural frequency and damping coefficient, which affect how faithfully it reproduces the true arterial pressure waveform.
What Is Damping?
Damping is the tendency of the monitoring system to dissipate the energy of pressure oscillations. Think of it like a shock absorber: a properly damped system faithfully follows the input signal, an overdamped system sluggishly smooths out the peaks and valleys, and an underdamped system rings and oscillates, overshooting the true pressure.
The monitoring system acts as a second-order harmonic oscillator with a natural frequency and a damping coefficient. The goal is a natural frequency above 25 Hz (high enough to reproduce all clinically relevant frequency components of the arterial waveform) and a damping coefficient between 0.5 and 0.7 (the optimal range for faithful signal reproduction).
Overdamping
An overdamped arterial line shows a waveform that looks blunted and sluggish:
- The systolic peak is underestimated (reads lower than true)
- The diastolic pressure is overestimated (reads higher than true)
- The dicrotic notch is absent or barely visible
- The waveform has a rounded, smooth appearance lacking sharp features
- Mean arterial pressure (MAP) is usually still accurate
Common causes of overdamping:
- Air bubbles in the tubing or transducer
- Blood clot (partial or complete) in the catheter
- Compliant (soft) tubing
- Excessive tubing length
- Kinked catheter or tubing
- Loose connections introducing air into the system
- Catheter tip against the arterial wall
Clinical impact: Overdamping underestimates systolic pressure, potentially masking hypertensive emergencies, and overestimates diastolic pressure, potentially masking hypotension. MAP remains approximately correct because the energy removed from the systolic peak is redistributed to the diastolic phase.
Underdamping
An underdamped arterial line shows a waveform with exaggerated features:
- The systolic peak is overestimated (reads higher than true)
- The diastolic pressure may be underestimated (reads lower than true)
- The dicrotic notch may appear exaggerated or multiple "ringing" oscillations may follow the systolic peak
- The waveform looks spiky with high-frequency oscillations
- Pulse pressure appears artificially widened
Common causes of underdamping:
- Excessive tubing length (increases the system's natural frequency resonance)
- Stiff tubing (paradoxically, very stiff tubing with long runs can resonate)
- Patient factors: tachycardia (higher frequency content in the waveform approaches the system's natural frequency), hyperdynamic states
- Resonance between the monitoring system and the arterial pressure signal
Clinical impact: Underdamping overestimates systolic pressure, potentially triggering unnecessary treatment for apparent hypertension, and may underestimate diastolic pressure. MAP is usually accurate. The exaggerated systolic peak may exceed 200 mmHg in hyperdynamic patients with underdamped systems, triggering alarms that do not represent true physiology.
The Square Wave Test (Fast-Flush Test)
The square wave test is the bedside method for assessing the dynamic response of the arterial monitoring system. It takes 5 seconds to perform and immediately reveals whether the system is optimally damped, overdamped, or underdamped.
How to Perform the Test
- Activate the fast-flush valve on the transducer system (pull the pigtail or squeeze the fast-flush device). This delivers 300 mmHg of pressure from the pressurized flush bag directly to the transducer.
- Hold the flush for 1-2 seconds. The waveform on the monitor jumps to a high, flat square wave (approximately 300 mmHg).
- Release the flush quickly. Observe the oscillations that follow.
Interpreting the Results
Optimally damped (damping coefficient 0.5-0.7): After release, the waveform shows 1-2 rapid oscillations before returning to the baseline arterial waveform. The first oscillation overshoots slightly below the baseline, the second returns to or slightly above the baseline, and the waveform then stabilizes. This indicates the system faithfully reproduces the arterial signal.
Overdamped (damping coefficient > 0.7): After release, the waveform returns slowly to baseline with no oscillation or one sluggish oscillation. The square wave itself may have rounded corners rather than sharp edges. Intervention is needed: check for air bubbles, clots, kinks, or loose connections.
Underdamped (damping coefficient < 0.5): After release, the waveform shows 3 or more oscillations before settling, with progressively decreasing amplitude (ringing). The more oscillations, the more underdamped the system. Intervention: reduce tubing length, remove unnecessary stopcocks, or add a damping device if available.
When to Perform the Square Wave Test
- At the beginning of each shift
- After any changes to the tubing system (adding stopcocks, extensions, or transducer)
- When waveform morphology appears abnormal
- When numerical values seem inconsistent with clinical status
- After changing the patient's position
- After any disconnection or flushing of the system
Common Arterial Line Artifacts and Troubleshooting
Catheter Whip (Catheter Fling)
When the arterial catheter tip moves freely within the artery (often in larger arteries like the femoral), the acceleration of the catheter itself generates pressure artifacts superimposed on the true waveform. This appears as high-frequency spikes, particularly prominent during systole. Catheter whip is more common with longer catheters and in hyperdynamic states. It can be reduced by ensuring the catheter is well-secured and appropriately sized.
Respiratory Variation
Normal respiratory variation in arterial pressure manifests as cyclical changes in systolic pressure with breathing. During spontaneous inspiration, intrathoracic pressure decreases, venous return to the right heart increases, but left ventricular stroke volume transiently decreases (due to the 2-3 beat transit time through the pulmonary circulation), causing systolic pressure to drop slightly. This is normal and is quantified as systolic pressure variation (SPV).
Exaggerated respiratory variation (SPV > 10 mmHg or pulse pressure variation > 13%) suggests hypovolemia and fluid responsiveness. This has become an important hemodynamic parameter in perioperative and critical care medicine.
Aortic Valve Artifact
In patients with mechanical aortic valves, the opening and closing of the prosthetic valve can produce high-frequency pressure transients that appear as spikes on the arterial waveform. These are not true pressure changes in the peripheral artery but rather transmitted vibrations.
Damped or Absent Waveform
A completely flat or very low-amplitude waveform suggests catheter occlusion (clot or kink), disconnection, or transducer malfunction. The first step is to attempt a gentle aspiration, then a flush. If the waveform does not return, the system should be systematically inspected from catheter to transducer.
Electrical Interference
60 Hz (or 50 Hz) electrical interference appears as a fine, regular oscillation superimposed on the waveform. It is caused by electromagnetic interference from nearby equipment and can be resolved by checking grounding connections and moving interfering devices.
Arterial Line Waveforms vs. PPG Waveforms: What Transfers
The arterial line and PPG waveform are related but fundamentally different signals. Understanding their relationship helps both ICU clinicians who also see PPG data and PPG researchers who reference invasive pressure as the ground truth.
Both waveforms reflect the same cardiac cycle events. The systolic upstroke in the arterial line corresponds to the rising edge of the PPG pulse. The dicrotic notch appears in both (though it is often less distinct in PPG). Heart rate, beat-to-beat interval variability, and basic rhythm information are identical between them.
The timing of fiducial points, such as the foot of the waveform, the systolic peak, and the dicrotic notch, correlates strongly between simultaneously recorded arterial line and PPG signals (r > 0.95 for timing, lower for amplitude features).
Where They Differ
Physical quantity measured. The arterial line measures intravascular pressure (mmHg). PPG measures changes in blood volume (arbitrary units, related to light absorption). Pressure and volume are related through arterial compliance, but the relationship is nonlinear and varies across individuals and conditions.
Waveform shape. The PPG waveform is the volume-time integral of the arterial pressure waveform, filtered by the compliance of the vascular bed. This means PPG waveforms are smoother, with rounder peaks and a less distinct dicrotic notch compared to arterial line tracings. High-frequency components of the pressure waveform are attenuated in the PPG.
Amplitude information. Arterial line amplitude is calibrated in mmHg. PPG amplitude is uncalibrated and depends on sensor placement, skin pigmentation, tissue thickness, and light source intensity. This means PPG can track relative changes in pulse amplitude but cannot directly provide absolute blood pressure values.
Measurement site. Arterial lines are typically placed in the radial, femoral, or dorsalis pedis arteries. PPG is measured from capillary beds in the fingertip, earlobe, or wrist. The capillary bed acts as a low-pass filter, further smoothing the waveform.
Response to hemodynamic changes. Both signals respond to the same cardiovascular events, but with different sensitivity. PPG amplitude is more sensitive to sympathetic vasoconstriction (which constricts the peripheral vascular bed) than arterial line amplitude. Conversely, arterial line waveforms more faithfully represent central hemodynamic changes because the catheter tip sits in a major artery.
For a detailed side-by-side comparison, see our PPG vs arterial blood pressure comparison guide.
Clinical Features That Transfer
Several clinically useful features can be assessed from both arterial line and PPG waveforms:
- Heart rate and rhythm: Both provide beat-by-beat heart rate with identical accuracy.
- Respiratory variation: Both show respiratory-induced cyclical variation that correlates with fluid responsiveness.
- Dicrotic notch position: The relative position of the dicrotic notch on the descending limb reflects similar vascular resistance information in both waveforms.
- Pulse contour abnormalities: Patterns like pulsus alternans (alternating amplitude) transfer well from arterial line to PPG. Pulsus bisferiens is sometimes visible in PPG but requires high signal quality.
- Heart rate variability: Beat-to-beat interval analysis is identical between R-R intervals derived from arterial line or PPG peak detection.
Features That Do Not Transfer
- Absolute blood pressure values: PPG cannot directly provide systolic, diastolic, or mean arterial pressure without calibration or algorithmic estimation.
- Precise notch morphology: The dicrotic notch is sharper and more reliable in arterial line tracings. PPG-based notch analysis requires careful signal quality assessment.
- High-frequency waveform components: Resonance artifacts (underdamping oscillations) in arterial lines have no PPG equivalent because PPG measures a fundamentally different physical quantity.
- Square wave test: There is no PPG equivalent to the fast-flush test for assessing monitoring system dynamics.
Understanding the cardiac cycle phases as they appear in PPG is covered in our PPG cardiac cycle phases guide. For methods of decomposing the PPG waveform into its constituent components, see our PPG waveform decomposition guide.
Reading the Arterial Waveform: A Systematic Approach
When approaching an arterial line waveform on a bedside monitor, a systematic assessment ensures nothing is missed:
Step 1: Check the system. Perform a square wave test. Confirm the waveform is optimally damped before interpreting it.
Step 2: Confirm leveling. Verify the transducer is level with the phlebostatic axis. A transducer that has shifted position will produce consistently erroneous readings.
Step 3: Assess the upstroke. Is it sharp (normal) or slurred (aortic stenosis)? Is it excessively steep (high output, AR)?
Step 4: Read the systolic peak. Note the value. Compare with cuff pressure if available. A discrepancy exceeding 15 mmHg warrants investigation (cuff error, damping issue, or peripheral amplification).
Step 5: Find the dicrotic notch. Is it present and well-defined (normal)? Absent (overdamping, AR, or severe stiffness)? Exaggerated (underdamping)?
Step 6: Assess diastolic runoff. Is it gradual (normal) or steep (low SVR, AR)?
Step 7: Look for variability. Check for respiratory variation (fluid status assessment), alternating amplitudes (pulsus alternans, LV failure), or irregular rhythms.
Step 8: Compare with clinical context. Does the waveform match what you expect based on the patient's condition, medications, and hemodynamic goals?
Frequently Asked Questions
What does a normal arterial line waveform look like?
A normal arterial line waveform shows a sharp, steep systolic upstroke (anacrotic limb) rising to a clear systolic peak, followed by a descending limb with a visible dicrotic notch about two-thirds of the way down, and then a gradual diastolic runoff to the end-diastolic pressure. The waveform is smooth without high-frequency oscillations, and the dicrotic notch is distinct but not exaggerated.
How do you tell if an arterial line is overdamped or underdamped?
Perform the square wave test (fast-flush test). After releasing the fast flush, count the oscillations: 1-2 oscillations before return to baseline is optimal, no oscillations means overdamped, and 3 or more oscillations means underdamped. Overdamped waveforms look blunted with low systolic peaks and absent dicrotic notch. Underdamped waveforms look spiky with exaggerated peaks and possible ringing artifacts.
What is the square wave test for arterial lines?
The square wave test (also called the fast-flush test) assesses the dynamic response characteristics of the arterial monitoring system. You activate the fast-flush device for 1-2 seconds, creating a high-pressure square wave on the monitor, then release it quickly and observe the oscillation pattern. The test reveals whether the system is optimally damped, overdamped, or underdamped, which determines whether the displayed pressure values are reliable.
Why does the arterial line systolic pressure differ from a blood pressure cuff?
Several factors cause discrepancies. Peripheral amplification makes radial arterial systolic pressure 5-15 mmHg higher than central aortic pressure. Underdamped systems can add another 10-30 mmHg to the reading. Cuff measurements themselves have inherent inaccuracy of 5-10 mmHg. The arterial line typically provides beat-by-beat values while the cuff provides intermittent measurements. A difference of up to 10-15 mmHg is generally accepted; larger discrepancies should be investigated.
How does a PPG waveform compare to an arterial line waveform?
Both show the same cardiac cycle events, but PPG measures blood volume changes (not pressure) and is recorded from the capillary bed (not a major artery). The PPG waveform is smoother with less distinct features. The systolic upstroke is gentler, the dicrotic notch is less sharp or absent, and amplitude is uncalibrated. Heart rate and timing features transfer accurately between the two. Morphological features like the dicrotic notch and respiratory variation are present in both but are less reliable in PPG.
What causes loss of the dicrotic notch on an arterial waveform?
The dicrotic notch can be lost due to monitoring system problems (overdamping from air bubbles, clots, or compliant tubing) or genuine physiological changes (severe aortic regurgitation, severe arterial stiffness, or extreme tachycardia where the diastolic period is too short for the notch to develop). Always perform a square wave test to rule out overdamping before attributing absent notch to physiology.
Can you assess fluid responsiveness from an arterial line waveform?
Yes. Respiratory variation in the arterial waveform is a validated predictor of fluid responsiveness in mechanically ventilated patients. Pulse pressure variation (PPV) greater than 13% or systolic pressure variation (SPV) greater than 10 mmHg suggests the patient will increase cardiac output in response to fluid administration. These thresholds apply only in patients on controlled mechanical ventilation without spontaneous breathing efforts and without cardiac arrhythmias.