Venous Pulsation Effects on PPG Signals: Sources, Mechanisms, and Mitigation
**Venous blood pulsations are an underappreciated source of error in photoplethysmography that can reduce SpO2 accuracy by 2-8 percentage points and d...
Venous blood pulsations are an underappreciated source of error in photoplethysmography that can reduce SpO2 accuracy by 2-8 percentage points and distort waveform morphology used for advanced cardiovascular assessment. The standard PPG signal model assumes that all pulsatile light absorption originates from arterial blood, but this assumption breaks down in multiple clinical and physiological scenarios where venous blood exhibits significant pulsatility. This article examines the origins of venous pulsations, their quantitative impact on PPG measurements, and strategies for detection and correction.
For foundational context on PPG signal generation and the assumptions underlying standard measurements, see our introduction to PPG technology.
The Arterial-Only Assumption in PPG
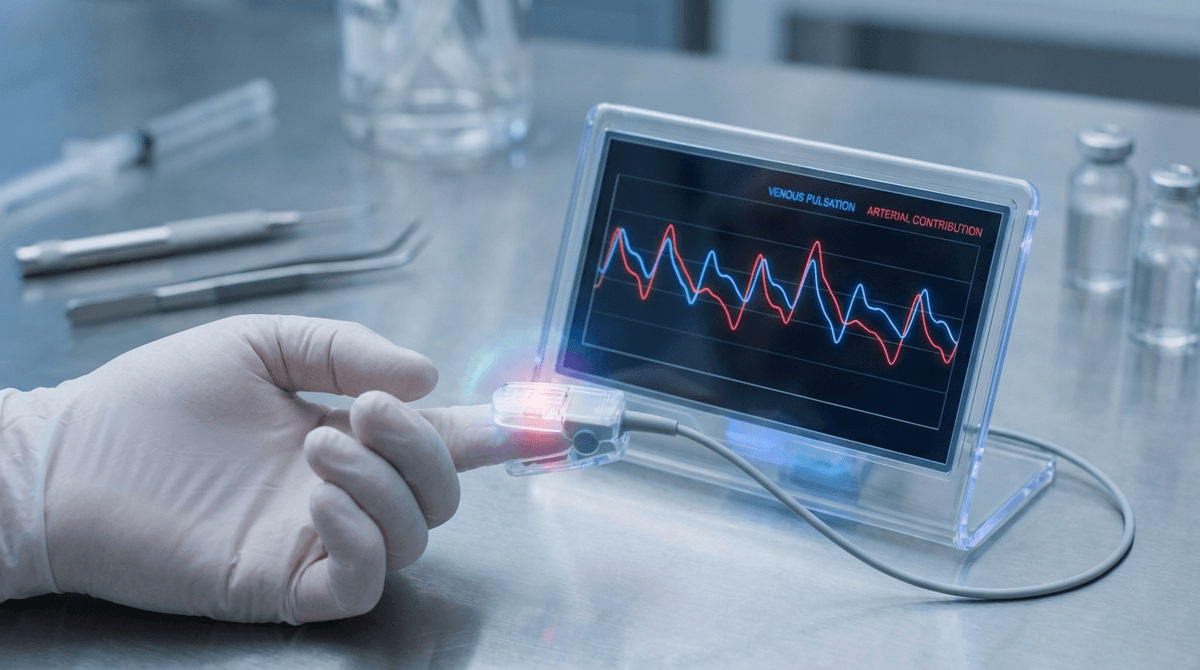
Conventional PPG theory rests on a critical assumption: the pulsatile (AC) component of the optical signal arises exclusively from arterial blood volume changes driven by the cardiac cycle. The non-pulsatile (DC) component is attributed to the constant absorption of tissue, bone, pigmentation, venous blood, and the non-pulsatile fraction of arterial blood.
This partition is fundamental to pulse oximetry. The SpO2 calculation relies on the ratio of pulsatile absorbance at two wavelengths (typically red 660nm and infrared 940nm), and this ratio is interpreted as reflecting arterial oxygen saturation because only arterial blood is assumed to pulsate. If venous blood also contributes to the pulsatile signal, the measured ratio becomes a weighted average of arterial and venous absorption characteristics, and the resulting SpO2 value no longer represents arterial saturation alone.
As Shelley (2007; DOI: 10.1213/01.ane.0000269512.82628.c3) noted in a seminal review, the arterial-only assumption is an approximation that holds reasonably well under normal physiological conditions but fails in several clinically important scenarios. Understanding when and why it fails is essential for interpreting PPG data correctly, particularly for SpO2 measurement applications.
Sources of Venous Pulsations
Venous blood can exhibit pulsatile behavior through several distinct physiological mechanisms, each with characteristic frequency content, amplitude, and clinical significance.
Right Heart Pressure Transmission
The right atrium generates a complex pressure waveform during the cardiac cycle, composed of the a-wave (atrial contraction), c-wave (tricuspid valve bulging during isovolumetric ventricular contraction), x-descent (atrial relaxation), v-wave (passive atrial filling during ventricular systole), and y-descent (early ventricular filling after tricuspid valve opening). These pressure fluctuations propagate retrograde through the venous system.
In healthy individuals, the venous pressure waveform is heavily damped by venous compliance and is barely detectable in peripheral veins. However, in pathological conditions, venous pulsations become dramatically amplified. Tricuspid regurgitation produces large systolic v-waves that transmit to peripheral veins. Shelley et al. (2005; DOI: 10.1213/01.ANE.0000153305.92608.A1) documented PPG-visible venous pulsations in 8 patients with significant tricuspid regurgitation, with venous pulsatile amplitudes reaching 20-50% of the arterial pulsatile amplitude. The resulting SpO2 readings were 3-7% below simultaneously measured arterial blood gas values.
Constrictive pericarditis and cardiac tamponade, which impair cardiac filling and elevate venous pressures, also generate prominent venous pulsations. Right heart failure with elevated central venous pressure increases venous distension and the transmission of cardiac-frequency pressure oscillations to the periphery.
Respiratory Modulation of Venous Flow
Respiration is the most common source of venous pulsations in the PPG signal. During inspiration, the decrease in intrathoracic pressure increases the pressure gradient between peripheral veins and the right atrium, accelerating venous return. During expiration, the gradient decreases and venous return slows. This respiratory cycling of venous volume creates a pulsatile component in the PPG signal at the respiratory frequency (typically 0.15-0.5 Hz, corresponding to 9-30 breaths per minute).
Alian et al. (2014; DOI: 10.1213/ANE.0000000000000289) quantified respiratory-induced venous pulsations in the finger PPG of 42 subjects and found that the respiratory component amplitude averaged 8-15% of the cardiac AC amplitude during normal tidal breathing, increasing to 25-40% during deep breathing. The respiratory venous component was particularly prominent in subjects with higher central venous pressure or during positive-pressure mechanical ventilation, where inspiratory increases in intrathoracic pressure impede venous return and amplify the respiratory venous oscillation.
Gravitational and Postural Effects
Body posture and limb position relative to heart level significantly influence venous pulsation magnitude. When the measurement site is below heart level, hydrostatic pressure increases venous distension, making veins more compliant and more susceptible to transmitting pressure pulsations. Additionally, gravitational venous pooling increases the venous blood volume within the optical interrogation region, amplifying the venous contribution to the PPG signal.
Reisner et al. (2008; DOI: 10.1097/ALN.0b013e31816c89e1) demonstrated that finger PPG signal quality and SpO2 accuracy were significantly affected by hand position relative to heart level. With the hand 30 cm below heart level, the venous contribution to pulsatile absorption increased measurably, and SpO2 readings dropped by 1-3% compared to the hand-at-heart-level baseline. This finding has practical implications for pulse oximetry protocols: accurate readings require the measurement site to be approximately at heart level.
Sensor Contact Pressure Effects
External compression from the PPG sensor attachment can create or amplify venous pulsations by partially obstructing venous outflow while permitting arterial inflow. This creates a tourniquet-like effect where venous blood accumulates during systole (when arterial inflow increases) and partially drains during diastole, producing a venous pulsatile component synchronized with but morphologically different from the arterial pulse.
Teng and Zhang (2006; DOI: 10.1088/0967-3334/27/12/007) investigated the effect of contact pressure on fingertip PPG signal characteristics and found that at moderate pressures (50-100 mmHg), the PPG AC amplitude was maximized due to improved optical coupling. At higher pressures (>120 mmHg), venous congestion began to occur, distorting the pulse waveform and introducing a secondary pulsatile component. Excessively tight sensor attachments, including overly snug wrist bands on consumer wearables, can produce similar effects. For guidance on how sensor design affects signal quality, see our PPG signal processing overview.
Quantitative Impact on SpO2 Measurement
The venous contamination effect on SpO2 can be modeled quantitatively. Standard pulse oximetry calculates the ratio R:
R = (AC_red / DC_red) / (AC_IR / DC_IR)
Where AC and DC represent the pulsatile and non-pulsatile components at red (660nm) and infrared (940nm) wavelengths, respectively. SpO2 is then derived from R using an empirical calibration curve.
When venous blood contributes a fraction f of the total pulsatile signal, the measured AC at each wavelength becomes a weighted sum of arterial and venous contributions:
AC_measured = (1-f) * AC_arterial + f * AC_venous
Because venous blood has lower oxygen saturation (typically SvO2 = 70-75%) than arterial blood (SaO2 = 95-99%), the venous contribution shifts the red/infrared ratio upward (toward lower saturation values on the calibration curve). The magnitude of the SpO2 error depends on both the venous fraction f and the difference between arterial and venous saturation.
Goldman et al. (2000; DOI: 10.1097/00000542-200011000-00030) modeled this effect and showed that a 10% venous contribution to the pulsatile signal produces approximately 2-3% SpO2 underestimation when true SaO2 is 97%. A 30% venous contribution produces 5-8% underestimation. The error is nonlinear and becomes larger when the arteriovenous saturation difference is greater (e.g., during exercise when SvO2 drops to 40-50% while SaO2 remains high).
Clinical Significance
In clinical settings, venous pulsation-induced SpO2 errors are most consequential in patients where accurate SpO2 monitoring is most critical. Patients with right heart failure, tricuspid regurgitation, or elevated central venous pressure are simultaneously at risk for venous pulsation artifacts and most likely to have true hypoxemia that needs to be accurately detected. The false low readings from venous pulsations can trigger unnecessary oxygen therapy, ICU admissions, or diagnostic workups.
Conversely, in scenarios where SvO2 is unusually high (e.g., sepsis with pathological arteriovenous shunting, where SvO2 may exceed 80%), venous pulsations would have a minimal effect on SpO2 accuracy because the arteriovenous saturation difference is small.
Impact on Waveform-Based Measurements
Beyond SpO2, venous pulsations affect the morphological features of the PPG waveform that are used for advanced measurements including blood pressure estimation and vascular assessment.
Dicrotic Notch Distortion
The dicrotic notch, which encodes information about aortic valve closure and wave reflections, can be obscured or shifted by superimposed venous pulsations. When the venous pulsation is at the cardiac frequency (as in tricuspid regurgitation), the venous v-wave can overlap temporally with the arterial dicrotic notch region, either masking the notch or creating a false secondary peak. This distorts derived metrics like the augmentation index and reflection index that depend on accurate notch identification, as discussed in our PPG waveform decomposition guide.
Pulse Amplitude Modulation
Respiratory venous pulsations produce baseline amplitude modulation of the PPG signal that can be confused with respiratory-induced modulation of the arterial signal. Both mechanisms produce oscillations at the respiratory frequency, but they have different physiological origins and implications. Arterial respiratory modulation reflects stroke volume variation through the Frank-Starling mechanism, which is clinically useful for assessing fluid responsiveness in ventilated patients. Venous respiratory modulation reflects venous compliance and right heart function. Failure to distinguish between these sources can lead to incorrect physiological interpretation.
Pulse Transit Time Errors
Venous pulsations can shift the apparent timing of PPG waveform features, particularly the foot and maximum slope of the systolic upstroke. If the venous pulsation adds or subtracts from the arterial signal near the upstroke region, the detected pulse onset time shifts, introducing errors in pulse transit time (PTT) measurements. Since PTT is used to estimate beat-to-beat blood pressure changes, venous contamination can degrade the accuracy of PPG-based blood pressure monitoring approaches.
Detection Methods
Identifying the presence and magnitude of venous pulsations in a PPG signal is challenging because they overlap spectrally and temporally with the arterial signal in many scenarios.
Multi-Wavelength Analysis
Exploiting the different optical absorption properties of arterial and venous blood at multiple wavelengths is the most promising detection approach. Because arterial blood (SaO2 approximately 97%) and venous blood (SvO2 approximately 75%) have different hemoglobin saturation levels, their red/infrared absorption ratios differ. If the pulsatile signal at the cardiac frequency contains both arterial and venous components, the measured R-ratio will be intermediate between the pure arterial and pure venous values.
Shafqat et al. (2015) proposed a three-wavelength PPG approach using green (525nm), red (660nm), and infrared (940nm) LEDs. The green channel, with its shallow penetration depth (1-2mm), is less affected by deeper venous pulsations and provides a primarily arterial reference. Comparing the timing and amplitude relationships across wavelengths can flag venous contamination. For more on how PPG wavelength selection affects signal composition, see our wavelength comparison guide.
Waveform Morphology Analysis
Venous pulsations often have distinct morphological characteristics from arterial pulsations. The right atrial waveform (a-wave, v-wave pattern) differs from the arterial systolic-diastolic pattern. When venous pulsations are at the cardiac frequency, they may produce a "double-peaked" or asymmetric distortion of the arterial pulse that can be detected through waveform shape analysis.
Cannesson et al. (2008; DOI: 10.1097/ALN.0b013e31816c89e1) showed that plethysmographic variability index (PVi), which quantifies the respiratory modulation of the PPG amplitude, is affected by venous pulsations. Large PVi values may reflect either arterial stroke volume variation (useful clinical information) or venous pulsation contamination (artifact). Distinguishing the two requires additional information such as central venous pressure or echocardiographic assessment.
Positional Provocation
A simple clinical test for venous pulsations is to raise the measurement site above heart level and observe whether the SpO2 reading or waveform morphology changes. Elevating the limb reduces venous distension and minimizes venous pulsatility. If the SpO2 reading increases by 2 or more percentage points when the hand is raised from below to above heart level, significant venous pulsation contamination is likely.
Correction Strategies
Several approaches have been proposed to correct for venous pulsation effects in PPG measurements.
Hardware Approaches
Applying gentle local pressure to compress superficial veins while preserving arterial flow can reduce venous pulsations. Some clinical pulse oximeter probes are designed with spring-loaded clips that apply sufficient pressure to partially occlude venous flow at the measurement site. However, excessive pressure can create its own artifacts, as discussed earlier, requiring a careful balance.
Measurement site selection also matters. The ear lobe, which has fewer veins and a simpler vascular anatomy than the fingertip, shows less venous pulsation contamination. Forehead reflectance pulse oximetry, positioned above heart level, is inherently less affected by gravitational venous pooling.
Algorithmic Approaches
Signal processing methods can attempt to separate arterial and venous components computationally. Independent component analysis (ICA) applied to multi-wavelength PPG data can potentially isolate arterial and venous sources based on their different spectral absorption signatures. Krishnan et al. (2008; DOI: 10.1109/TBME.2008.919714) applied ICA to two-wavelength PPG and demonstrated partial separation of arterial and venous pulsatile components in simulated and experimental data.
Adaptive filtering using a respiratory reference (from chest impedance or accelerometer-derived respiratory signal) can attenuate respiratory-frequency venous pulsations. However, this approach risks also removing the arterially-mediated respiratory modulation, which carries useful physiological information about fluid responsiveness.
Model-Based Correction
A more sophisticated approach uses a biophysical model that explicitly accounts for both arterial and venous pulsatile compartments. The model treats the measured PPG signal as a sum of arterial and venous components, each with its own pulsatile amplitude, oxygen saturation, and temporal dynamics. By fitting this model to multi-wavelength PPG data, both SaO2 and SvO2 can be estimated simultaneously, effectively turning the venous contamination problem into an opportunity for additional physiological measurement.
Franceschini et al. (1999; DOI: 10.1364/AO.38.003616) demonstrated this concept using near-infrared spectroscopy with multiple source-detector separations, simultaneously estimating arterial and venous oxygenation changes. Extending this approach to standard two-wavelength PPG is more constrained but feasible when combined with temporal signal analysis.
Practical Implications
For researchers and engineers working with PPG data, awareness of venous pulsation effects leads to several practical recommendations.
First, always note the measurement site position relative to heart level. For wrist PPG, arm position can vary significantly during daily wear, and SpO2 or waveform measurements from periods of arm-dependent positioning should be flagged or excluded.
Second, in clinical pulse oximetry, unexplained low SpO2 readings that do not match the patient's clinical presentation should prompt consideration of venous pulsation artifacts, especially in patients with known right heart disease or elevated central venous pressure.
Third, PPG waveform analysis algorithms should not assume that the dicrotic notch and diastolic wave originate purely from arterial wave reflection. In populations with significant venous pulsations, these features may be contaminated, and derived vascular indices should be interpreted cautiously.
Fourth, when validating PPG devices against reference standards, inclusion of patients with known venous pulsation sources (right heart failure, tricuspid regurgitation) is important for characterizing the full error distribution of the device, rather than validating only in the easy cases where the arterial-only assumption holds.
For further exploration of PPG signal quality challenges and processing strategies, visit our algorithms reference and PPG learning center.